Successful Outcome after Single Step Surgery for Portal Biliopathy
By Abu Bakar Hafeez Bhatti1, Eraj Sahaab1, Faisal Saud Dar1, Fazal Manan2Affiliations
doi: 10.29271/jcpsp.2020.04.453Sir,
Extra-hepatic portal vein obstruction (EHPVO) is the most common cause of gastrointestinal bleeding in children and young adults (68-84%).1 Portal biliopathy (PB) occurs in 77-100% patients with EHPVO.2 PB refers to cholangiographic abnormalities, which occur in patients with portal cavernoma. Timely intervention is important because there is a risk of secondary liver cirrhosis.3 Surgery is reserved for cases refractory to medical, endoscopic and radiological treatments. Surgical approach to PB remains evolving and conflicting.4 Here, we share our experience with a patient who underwent single-step surgery for PB.
A 19-year boy was referred to us with a diagnosis of PB. Past surgical history was significant for a laparoscopic cholecystectomy, complicated by troublesome bleeding. More recently, the patient underwent endoscopic retrograde cholangiopancreatography (ERCP) thrice for endoscopic stone removal. This led to hemobilia which was controlled with stent placement as no other intervention was possible. Serology was negative for hepatitis B and C. Thrombotic screen was negative and total bilirubin was 3.2 mg/dl. A liver dynamic CT showed choledocholithiasis, biliary dilatation, splenomegaly, varices and chronic portal vein thrombosis with non-visualisation of superior mesenteric vein (SMV).
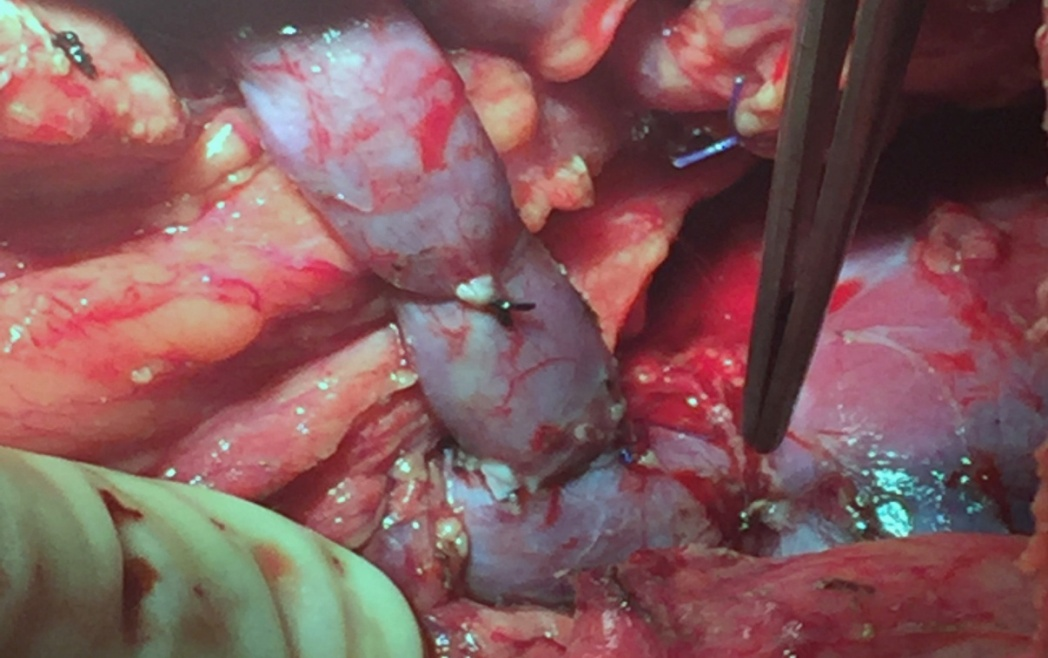
Figure 1: Proximal splenorenal shunt after splenectomy.
After discussion in multi-disciplinary team, he underwent splenectomy, proximal splenorenal shunt and T-tube repair for biliary drainage. Intra operative findings included extensive adhesions from previous surgery, splenomegaly with pericholedochal varices, choledocholithiasis and portal pressure of 19 cm of H2O. A splenectomy and splenorenal shunt reduced the portal pressure to 9 cm of H2O (Figure 1). For biliary drainage, choledochotomy, stone removal and T-tube repair was performed. He was discharged on 10th post operative day and T-tube was removed after 3 weeks. A CT scan, one month after surgery, showed patent splenorenal shunt and hepatic venous blood flow through a varix (Figure 2). Eight months after surgery, he is doing well with normal liver function tests (LFTs) with total bilirubin of 0.8 mg/dl.
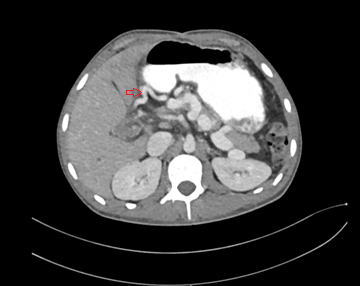
Figure 2: Post operative CT scan showing venous inflow to the liver through a varix (No portal flow).
Although controversial, it has been shown that first use of portal decompression is probably a better option for PB.2,5,6 There is only one case report demonstrating combined single-step treatment for PB with portosystemic shunt (PSS) and bilioenteric anastomosis.7 To the best of our knowledge, our case represents the first experience with combined PSS and T-tube repair for PB. There is reduced risk of damage to pericholedochal varices with T-tube repair, thus preserving blood flow to the liver. A normal intra-operative and week-3 cholangiogram mitigates the risk of an evolving biliary stricture. With hemobilia resolved and integrity of the bile duct preserved, future ERCP is possible in this patient, in case a stricture develops.
CONFLICT OF INTEREST:
Authors declared no conflict of interest.
AUTHORS’ CONTRIBUTION:
AHB: Planned and performed the surgical procedure, contributed to manuscript writing, and critical review.
FSD: Performed the surgery, and contributed to critical review.|
ES, FM: Contributed to literature review, preoperative management of patient and manuscript writing.
REFERENCES
- Arora A, Sarin SK. Multimodality imaging of primary extrahepatic portal vein obstruction (EHPVO): What every radiologist should know. Br J Radiol 2015; 88:20150008.
- Franceschet I, Zanetto A, Ferrarese A, Burra P, Senzolo M. Therapeutic approaches for portal biliopathy a systematic review. World J Gastroenterol 2016; 22:9909-20.
- Harmanci O, Bayraktar Y. How can portal vein cavernous transformation cause chronic incomplete biliary obstruction? World J Gastroenterol 2012; 18:3375-8.
- Lal R, Sarma MS, Gupta MK. Extra hepatic portal venous obstruction what should be the mainstay of treatment? Indian J Pediatr 2017; 84:691-9.
- Agarwal AK, Sharma D, Singh S, Agarwal S, Girish SP. Portal biliopathy a study of 39 surgically treated patients. HPB (Oxford) 2011; 13:33-9.
- Chattopadhyay S, Govindasamy M, Singla P, Varma V, Mehta N, Kumaran V, et al. Portal biliopathy in patients with non-cirrhotic portal hypertension does the type of surgery affect outcome? HPB (Oxford) 2012; 14:441-7.
- D'Souza MA, Desai D, Joshi A, Abraham P, Shah SR. Bile duct stricture due to caused by portal biliopathy treatment with one-stage portal-systemic shunt and biliary bypass. Indian J Gastroenterol 2009; 28:35-7.