Two Cases of Interrupted Inferior Vena Cava with Azygos / Hemiazygos Continuation
By Saerah Iffat Zafar1, Aliya Halim1, Waqas Khalid2, Mobeen Shafique1, Hina Nasir1Affiliations
doi: 10.29271/jcpsp.2022.08.S101ABSTRACT
Interrupted inferior vena cava (IVC) is a rare disease, occurring either in isolation or in association with asplenia or polysplenia syndromes. Infrahepatic part of the IVC is absent representing the failure of fusion of the vitelline and subcardinal embryological portions of the IVC. It is replaced by an enlarged azygos or hemiazygos vein continuing into the thorax, either into the superior vena cava or into the brachiocephalic veins. We present two cases of interrupted IVC, one occurring in isolation with hemiazygos continuation and discovered incidentally, and the second one is a child with azygos continuation, associated with polysplenia syndrome.
Key Words: Inferior vena cava, Polysplenia, Azygous vein, Hemiazygos vein.
INTRODUCTION
Interrupted inferior vena cava (IVC) with azygos or hemiazygos continuation is a rare anomaly occurring either in isolation or in association with other congenital anomalies.1,2 Infrahepatic part of the IVC is usually absent representing the failure of fusion of the vitelline and subcardinal embryological portions of the IVC. The infrahepatic part of the IVC is replaced by an enlarged azygos or hemiazygos vein continuing into the thorax, either into the superior vena cava or into the brachiocephalic veins. Herein, we present two cases of interrupted IVC, one occurring in isolation in an adult patient while the other in a child in association with situs ambiguous. These case reports pertain to an interrupted hepatic segment of IVC, with failure of fusion of its cranial and caudal parts.
CASE REPORT
CASE 1:
A 32-year asymptomatic male soldier presented to the unit’s medical center for his annual medical evaluation two months ago. He was non-hypertensive and non-diabetic. His annual routine electrocardiogram (ECG) revealed bradycardia with junctional escape rhythm.
Cardiac enzymes and other routine investigations were within normal limits. The exercise Tolerance Test (ETT) was borderline while echocardiography revealed good left ventricular function. His electrophysiological studies (EPS) were planned. Femoral venous access was attempted but the wire had an aberrant route. Left subclavian puncture also failed and the patient was sent to the radiology department for contrast-enhanced CT abdomen to rule out abnormality of IVC. CT showed only the cranial part of IVC draining hepatic veins before entering the right atrium (Figure 1). Infrahepatic part was atretic. Iliac and renal veins drained via distended hemiazygos vein within the abdomen, entering the thorax and draining into the left brachiocephalic vein. His final diagnosis was interrupted IVC with hemiazygos continuation draining ectopically into the left brachiocephalic vein. Considering the association of interrupted IVC with sinus nodal dysfunction, he is planned to have a permanent pacemaker.
CASE 2:
A 4-year child was referred to the radiology department for an ultrasound of the abdomen with complaints of persistent pain in the abdomen. She was found to have multiple masses in the right hypochondrium, enlarged liver, and ectopic right kidney. Her CT abdomen revealed a centrally placed liver and stomach and multiple splenic tissues in the right hypochondrium, and right pelvic kidney (Figure 2). Note was made of interrupted IVC which drained only the hepatic veins before entering the right atrium. Lower limb and renal veins drained into the azygos vein, which drained superiorly into the superior vena cava within the thorax. Based on these findings, a diagnosis of polysplenia with situs ambiguous, ectopic right kidney and interrupted IVC with azygos continuation was made.
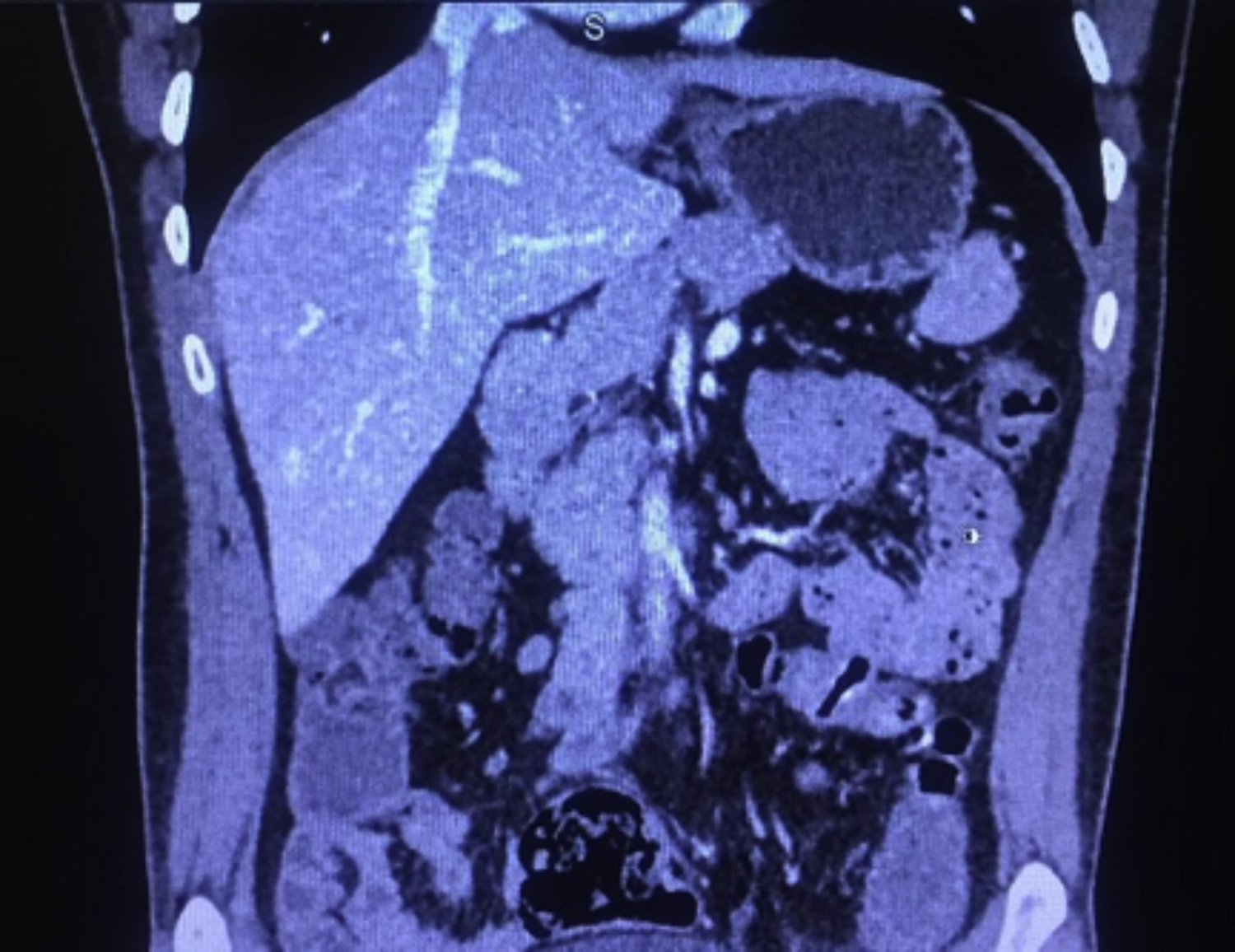 Figure 1: Hepatic segment of inferior vena cava draining hepatic veins and not continuing further caudally (case 1).
Figure 1: Hepatic segment of inferior vena cava draining hepatic veins and not continuing further caudally (case 1).
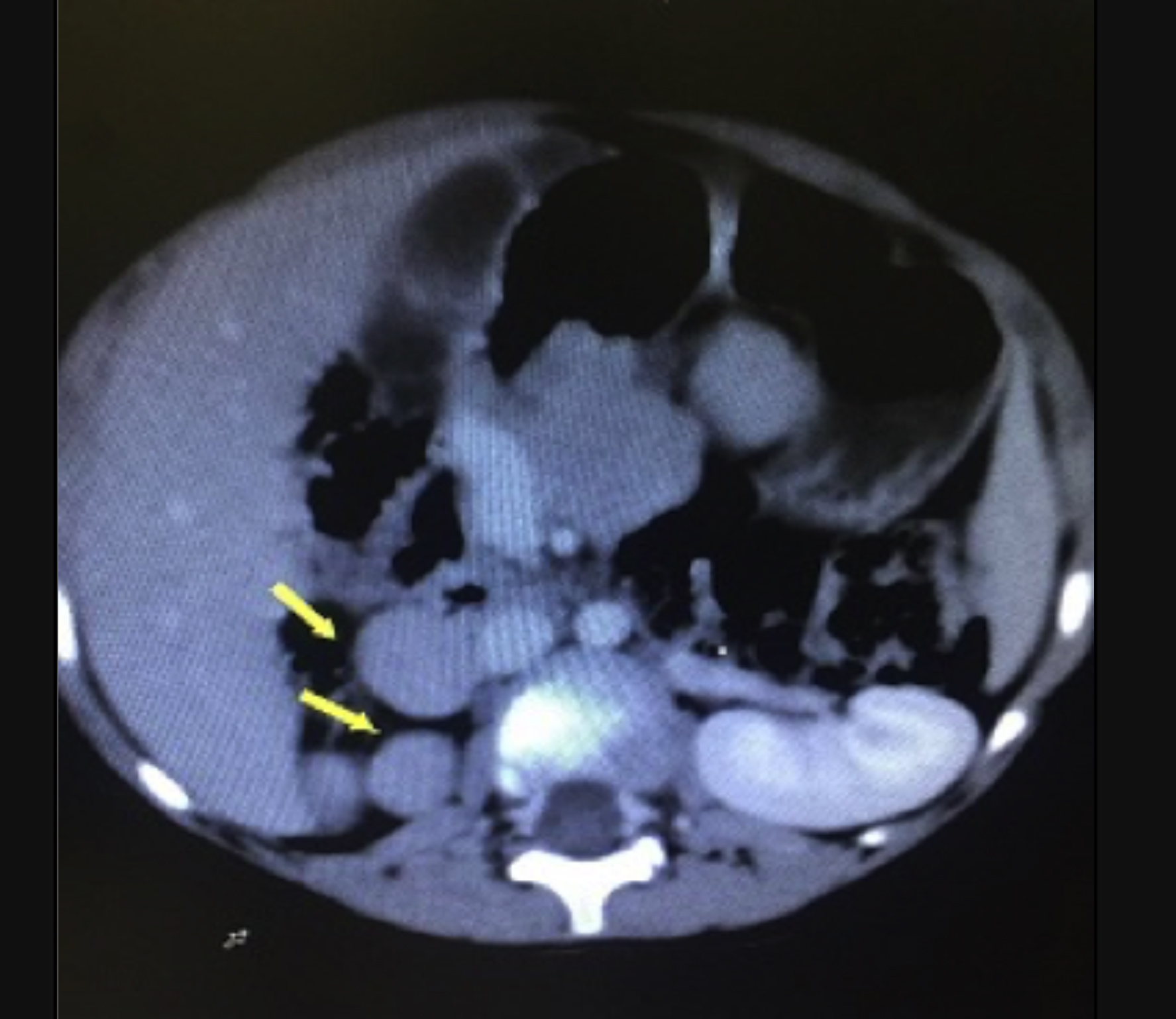 Figure 2: Polysplenia- multiple spleens are seen in the right hypochondrium (arrows), dilated azygos vein lying to the right of the aorta, replacing caudal part of inferior vena cava and absence of right kidney at its anatomical location (case 2).
Figure 2: Polysplenia- multiple spleens are seen in the right hypochondrium (arrows), dilated azygos vein lying to the right of the aorta, replacing caudal part of inferior vena cava and absence of right kidney at its anatomical location (case 2).
DISCUSSION
Interrupted IVC with azygos or hemiazygos continuation is a rare disorder occurring in 0.6-2% of the population with congenital heart disease; it is even rarer occurring in isolation at <0.3%.1 In approximately 90% of patients, it appears as an isolated anomaly2 causing no symptoms; such patients remain undiagnosed in their earlier life and the disease may be discovered as part of investigation for some other cause or in investigations for failed vascular interventions. While the congenital variety is associated with situs inversus or situs ambiguous with polysplenia, this disease is rare with an incidence of 1:1400 - 1:35000.3 At younger age, interrupted IVC acts as a predisposing factor for deep venous thrombosis of lower limbs without any abnormality of coagulation factors.4 Other symptoms include leg varices, hepatic vein thrombosis, and hematochazia.5 A case series on inferior vena cava anomalies in Pakistan reported one case of interrupted IVC with multiple collaterals and enlarged azygos and hemiazygos veins occurring in a 19-year-old boy with varicose veins in both lower limbs without evidence of deep venous thrombosis.6 Association with sinus node dysfunction is also known especially in conjunction with left isomerism, which includes the absence of hepatic segments of IVC, midline liver, and polysplenia; 70% of patients present with bradycardia around 15 years of age.7
Interrupted IVC with azygos or hemiazygos continuation is a rare, probably underdiagnosed anomaly, especially when occurring in isolation as the patients are asymptomatic. When occurring in association with polysplenia or asplenia syndromes, patients are discovered at younger age on account of early cardiac complications. Knowledge of these anomalies is important in planning of right heart catheterization, EPS, cardiopulmonary bypass, or IVC filter placement.
PATIENTS’ CONSENT:
Due consents from the patients were taken for the publication of their medical information.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
SIZ: Corresponding author.
AH: Collection of data of patients and their follow up.
WK: Cardiology work up information.
MS: Helping in content writing.
HN: Help in references, content.
All the authors approved the final version of the manuscript to be published.
REFERENCES
- Yilmaz E, Gulcu A, Sal S, Obuz F. Interruption of the inferior vena cava with azygos/hemiazygos continuation accompanied by distinct renal vein anomalies: MRA and CT assessment. Abdom Imaging 2003; 28(3):392-4. doi 10.1007/s00261-002-0031-5.
- Hardwick T, Belcher E, Sabharwal T, King J. Interrupted inferior vena cava: high risk anatomy for right thoracotomy. Interactive CardioVascular and Thoracic Surgery 2011; 12(5):850-2. doi: 10.1510/icvts.2010. 258731.
- Kwon SH, Shin SY. Incidental adult polysplenia with situs inversus, interrupted inferior vena cava with azygos continuation, patent ductus arteriosus, and aortic branches variations: A case report. J Thoracic Disease 2018; 10(2):E138-41. doi: 10.21037/jtd.2018.01.128.
- Angelika NF, Furthner D, Lanzersdorfer R, Sekyra P, Hinterreiter F. Interrupted inferior vena cava and deep venous thrombosis- an underdiagnosed pediatric disease. Pediat Therapeut 2014; 4:206. doi: 10.4172/2161-0665. 1000206.
- Koc Z, Oguzurt L. Interruption or congenital stenosis of the inferior vena cava: Prevalence, imaging, and clinical findings. Eur J Rad 2007; 62(2):257-66.doi: 10.1016/j. ejrad.2006.11.028.
- Baloch R, Kadri S, Ahmed N. Agenesis of inferior vena cava with cavernous transformation and hypoplastic infrarenal part of IVC, rare congenital vascular anomalies: A case series. J US-China Medical Sci 2016; 13:19-23. doi: 10.17265/1548-6648/2016.01.003.
- Gupta GM, Sarkar PG, Tayagi S. Complete heart block in an elderly patient with polysplenia syndrome: A case report. Interv Cardiol 2017; 10(1):9-11.