Simple Congenital Hamartoma of Retinal Pigment Epithelium
By Tayyaba Gul MalikAffiliations
doi: 10.29271/jcpsp.2022.04.31ABSTRACT
A 45-year female presented in the Outpatient Department of a tertiary care hospital of Lahore with dimness of vision in the right eye. Her history revealed that the patient had noticed decreased vision since her childhood. Fundus examination revealed a jet-black slightly raised lesion about the size of ¼-disc diameter, located in the centre of macula. Optical coherence tomography (OCT) showed a highly hyper-reflective lesion at the fovea with sharp steep shadowing of the underlying structures due to backscattering. We excluded congenital hypertrophy of the retinal pigment epithelium (CHRPE) from our differential diagnosis, as solitary CHRPE is a flat well-demarcated lesion at the level of retinal pigment epithelium (RPE). Adenoma of RPE was eliminated as it has a large feeding and draining blood vessels with intra- and sub-retinal exudation. Choroid and surrounding retina was normal in our patient, which was helpful in differentiating it from choroidal nevus/choroidal melanoma. Our final diagnosis was simple congenital hamartoma of RPE.
Key Words: Hamartoma, Retinal pigment epithelium, Macula.
INTRODUCTION
Simple congenital hamartoma of retinal pigment epithelium (CHRPE) is a rare tumour of retinal pigment epithelium (RPE), which was first reported by Laqua in 1981.1 Later in 1989, Gass described it as “retinal hamartoma” and reported 10 cases.2 During the last 37 years since its first description, only few cases have been described. The largest case series is by Shields et al.,3 who reported five cases. More cases are from the West and few from Asia, including India and Japan. Initial details regarding clinical features, ultrasonography, fundus fluorescein angiography (FFA), optical coherence tomography (OCT) and follow-up course, were also described by Shields et al.3 They described three patterns of this tumour; superficial retinal involvement, full thickness retinal involvement with pre-retinal extension, and full thickness involvement with intrinsic vascularisation.3
Simple hamartoma of RPE is a focal hyperplasia in contrast to congenital hypertrophy of RPE. There is dark black intra-retinal pigmentation, small size, macular location and slight elevation in the vitreous cavity. This case report is another addition to very few case reports of simple CHRPE.
CASE REPORT
A 45-year female presented in the Outpatient Department of a tertiary care hospital of Lahore with dimness of vision in the right eye. Her history revealed that the patient had noticed decreased vision since her childhood. The patient was non-diabetic, non-hypertensive, and there was no history of any other systemic disease, trauma or drug intake. Her family history was unremarkable.
On examination, her best-corrected visual acuity was 6/36 in the right eye and 6/6 in the left eye. Intra-ocular pressures were 16 mm and 18 mm Hg in the right and left eyes, respectively. Pupillary reactions were normal. She was orthotropic and extraocular movements were normal in both eyes. Slit-lamp examination showed no abnormality. Fundus examination revealed a jet-black slightly raised lesion about the size of ¼-disc diameter, located in the centre of macula. Cup to disc ratio was 0.3 on both sides. We advised spectral domain OCT (SD-OCT) (macular cube) to ascertain if there was any associated edema, exudation, epi-retinal membrane or sub-retinal fluid. OCT showed a highly hyper-reflective lesion at the fovea with sharp steep shadowing of the underlying structures due to backscattering. There was no associated macular edema, exudation, or sub-retinal fluid (Figure 1).
The differential diagnosis in our assessment was CHRPE, combined hamartoma of the retina and RPE, adenoma or adenocarcinoma of RPE, intra-retinal foreign body, and retinal invasion from an underlying choroidal nevus (melanocytoma) or choroidal melanoma.
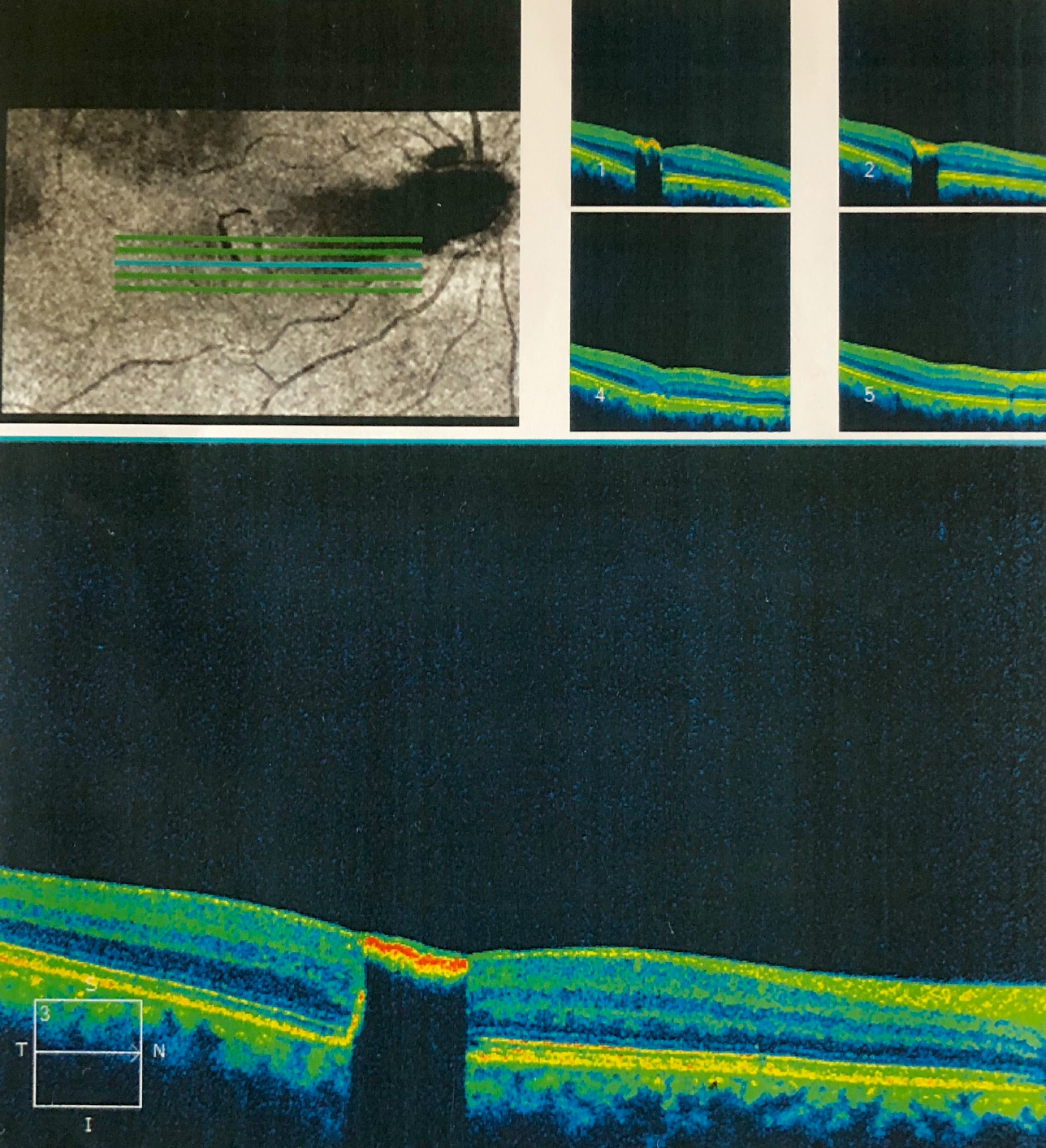 Figure 1: SD-OCT showing, 5-line Raster scan of SCHRPE at the fovea. The lesion is hyper-reflective with sharp and steep shadowing of the underlying retinal layers due to back scattering.
Figure 1: SD-OCT showing, 5-line Raster scan of SCHRPE at the fovea. The lesion is hyper-reflective with sharp and steep shadowing of the underlying retinal layers due to back scattering.
Intra-ocular foreign body was excluded, as there was no history of trauma. Combined hamartoma of retina and RPE is a full thickness retinal mass and has a vitreoretinal interface abnormality leading to tortuosity of the retinal vessels. On OCT, there was an irregular epi-retinal membrane with retinal thickening and cystic spaces. As these findings were absent in this case, combined hamartoma of retina and RPE was ruled out.
We excluded CHRPE from our differential diagnosis, as solitary CHRPE was flat well-demarcated lesion at the level of RPE. It is usually surrounded by a depigmented halo and sometimes a double halo pattern. The lacunae develop inside the lesion and eventually become completely depigmented. Such evolutionary changes have never been reported in simple CHRPE. Adenoma of RPE was excluded as it has a large feeding and draining blood vessels with intra- and sub-retinal exudation. Choroid and surrounding retina were normal in our patient, which was helpful in differentiating it from choroidal nevus/choroidal melanoma. Our final diagnosis was simple CHRPE.
DISCUSSION
Simple CHRPE appears as a focal, well-circumscribed, jet-black lesion, which is presumed to involve all retinal layers. Embryologically, it is derived from migration and proliferation of RPE cells into sensory retina. Its presentation is usually incidental in most of the cases unless it involves foveal region; as was the case with our patient. Most of the cases are less than 1 mm in diameter and are located within the macula. This particular case was also 0.25 disc diameter in its maximum dimension. Although all the cases reported so far were located in the macular region but there is a possibility that such lesions may also be present in the periphery and not reported because of peripheral location.
Few systemic and ocular associations of this tumour are also described in the literature. Our case was a solitary case without any systemic and ocular association. However, vitreo-macular traction has been described by some authors.4 More recently, a case of simple CHRPE was reported with macular edema.5 Another case has been described as associated with Coat’s disease.6 Similarly, only one case has been described with Down’s syndrome.7
As more and more cases are being reported globally, more characteristic features of this rare tumour are becoming evident. On ultrasonography, the tumour appears as an echogenic, nodular lesion on retina, with moderate to high internal reflectivity without shadowing.4 However, most of the times, the tumor is very small and is not detected with B-scan. In our case, the lesion was not detected on B-scan. FFA findings include blocked fluorescence and absence of leakage throughout the angiographic frames. Recently, histopathological features were described by Barnes et al.8 They reported a 66-year Hispanic female, who had simple CHRPE with vitreo-macular traction. She had to undergo pars plana vitrectomy (PPV). The lesion was excised during PPV. Histopathological examination revealed nodular proliferation of hyperplastic RPE cells.8 This tumour is different from the histopathological picture of combined hamartoma of retina and RPE as in combined hamartoma of retina and RPE. The RPE infiltration is seen into retina with gliosis, which is responsible for the wrinkling of the retina.
More recently, with the advent of optical coherence tomography angiography (OCTA), vascularity of the lesion has also been studied. Arjmand et al. described large-caliber vessels throughout the tumor, especially at the superficial and deep plexuses, but no blood flow was detected at the choriocapillaris level.9 Electrophysiological test was described by Ito et al., who reported no changes in the multifocal electroretinography (mfERG) of the patients with simple CHRPE. 10
Simple CHRPE is a rare finding. Not much literature is available on this entity. The largest case series available is of five cases. This case report is a contribution to the already very few existing reports.
The limitation of our report is that, as the diagnosis was confirmed clinically and on OCT, we did not perform FFA and OCTA because of the financial constraints of the patient. However, SD-OCT is a good diagnostic tool in differentiating simple CHRPE from other lesions of RPE.
PATIENT’S CONSENT:
Informed consent was obtained from the patient to publish the data concerning this case.
CONFLICT OF INTEREST:
The author declared no conflict of interest.
AUTHOR’S CONTRIBUTION:
TGM: Data collection, literature research, manuscript writing, and final review.
REFERENCES
- Laqua H. Tumors and tumor-like lesions of the retinal pigment epithelium. Ophthalmologica 1981; 183(1):34-8. doi: 10.1159/000309131.
- Gass JD. Focal congenital anomalies of the retinal pigment epithelium. Eye 1989; 3(P 1):1-18. doi: 10.1038/ eye.1989.2.
- Shields CL, Shields JA, Marr BP, Sperber DE, Gass JD. Congenital simple hamartoma of the retinal pigment epithelium: A study of five cases. Ophthalmol 2003; 110(5):1005-11. doi: 10.1016/S0161-6420(03)00087-3.
- Shukla D, Ambatkar S, Jethani J, Kim R. Optical coherence tomography in presumed congenital simple hamartoma of retinal pigment epithelium. Am J Ophthalmol 2005; 139(5): 945-7.doi: 10.1016/j.ajo.2004.11.037.
- Bach A, Gold AS, Villegas VM, Wildner AC, Latiff A, Ehlies FJ, et al. Simple hamartoma of the retinal pigment epithelium with macular edema. Optom Vis Sci 2015; 92(4 Suppl 1):48-50.doi: 10.1097/OPX.0000000000000534.
- Heo WJ, Park DH, Shin JP. A case of congenital simple hamartoma of the retinal pigment epithelium and coats’ disease in the same eye. Korean J Ophthalmol 2015; 29(4): 282-3. doi: 10.3341/kjo.2015.29.4.282.
- Panagopoulos A, Chalioulias K, Murray AT. Bilateral congenital hamartomas of the retinal pigment epithelium in a patient with down's syndrome. Eye 2008; 22(5): 735-6. doi.org/10.1038/eye.2008.27.33
- Barnes AC, Goldman DR, Laver NV, Duker JS. Congenital simple hamartoma of the retinal pigment epithelium: clinical, optical coherence tomography, and histopatho-logical correlation. Eye (London) 2014; 28(6): 765-6. doi: 10.1038/eye.2014.49.
- Arjmand P, Elimimian EB, Say EAT, Shields CL. Optical coherence tomography angiography of congenital simple hamartoma of the retinal pigment epithelium. Retin Cases Brief Rep 2019; 13(4): 357-60. doi: 10.1097/ICB.00000 00000000596.
- Ito Y, Ohji M. Long-term follow-up of congenital simple hamartoma of the retinal pigment epithelium: A Case Report. Case Rep Ophthalmol 2018; 9(1):215-20. doi: 10.1159/000487631.