Granulomatous Inflammation of Greater Omentum Caused by a Migrating Fishbone
By Tao Fan1, Chao-Qi Wang2, Ying-Jie Song3, Wan-Yan Wu1, Ya-Nan Wei1, Xue-Tao Li1Affiliations
doi: 10.29271/jcpsp.2022.08.S124ABSTRACT
Fishbone is the most common ingested gastrointestinal foreign matter and is less than 1% perforate. However, a fishbone penetrating the gastrointestinal tract and causing granulomatous inflammation of the greater omentum with local suppuration is not common. Because of the nonspecific clinical symptoms, gastrointestinal perforation may be manifested only as dull abdominal pain, which is often ignored and timely clinical treatment may be delayed. We report a case of a 61-year male who experienced intermittent right median ventral abdominal pain for half a year. These symptoms were the result of granulomatous inflammation of the greater omentum with local suppuration caused by a migrating fishbone (3.5 cm in length). Finally, the fishbone was removed by exploratory laparotomy.
Key Words: Fishbone, Gastrointestinal perforation, Greater omentum, Granulomatous inflammation, Laparotomy.
INTRODUCTION
The esophagus and gastrointestinal tract are sometimes penetrated or perforated by ingested foreign bodies such as needles, fishbones, etc.1,2 Although most of the ingested foreign bodies pass through the esophagus and gastrointestinal tract smoothly, approximately 10% to 20% need to be removed by endoscopy, and about 1% need surgery.3 An ingested fishbone penetrating the esophagus or gastrointestinal tract and causing granulomatous inflammation with local suppuration is a very rarely reported phenomenon.
Herein, we present a case of an ingested fishbone that was removed by laparotomy, and which caused granulomatous inflammation of the greater omentum with local suppuration.
CASE REPORT
A 61-year male presented to our institution complaining of intermittent right median ventral abdominal pain for six months which aggravated for the last three days. The patient had a history of appendectomy more than 20 years ago but no significant family history.
On admission, the temperature was 36.8℃, the heart rate was100 beats/min, the blood pressure was 135/90 mmHg, the respiratory rate was 21 breaths/min, and the oxygen saturation was 97% on ambient air. In the abdominal examination, a 10×10 cm mass was palpable in the right abdomen, with positive tenderness and no rebound pain. In the laboratory tests, white blood cell count was 9100/mm3, C-reactive protein, 8.13 mg/dl, red blood count, 437×104/mm3, and amylase, 72 IU/L. There were no other abnormalities, including occult blood in the stool, or elevated tumor markers. Chest radiography showed no abnormalities. Abdominal radiography showed a linear calcified structure about 3.5 × 0.2 cm in the right abdomen (Figure 1A), and no free gas under the diaphragm. Abdominal ultrasonography showed intestinal echo in the right mid-clavicular line in the abdominal cavity at the level of the umbilical horizontal line (Figure 1B). A magnetic resonance imaging (MRI) scan of the abdomen showed a linear, dense foreign body, seemingly penetrating from the anterior wall of the gastric antrum. The abnormal signal on the right side of the abdomen, likely inflammatory in origin with the formation of the encapsulated abscess was also observed (Figure 1C). Following the review of the whole case and consideration of extraneous matter ingestion, the patient remembered eating fish 6 months back.
In the beginning, we attempted to remove the foreign object with an endoscope but failed because it was not found. Afterward, an exploratory laparotomy was performed on the 6th hospitalisation day, which revealed a large mass wrapped in the greater omentum. We carefully dissociated the greater omentum, gastrointestinal tract, and pancreas, and found a fishbone of approximately 3.5 cm in length wrapped in the greater omentum (Figure 2A). Because the leak of the penetrated gastric wall was not detected during the operation, we did not perform gastric wall-related suture repair. The fishbone was successfully removed, and intravenous cefuroxime was used for five days. On gross examination, the foreign matter was identified as a 3.5 cm long fishbone (Figure 2B). Histopathological findings revealed an inflammatory response around the fishbone involving the greater omentum (Figure 2C).
The patient's pain improved after surgery and he was discharged home on the 10th postoperative day without any complications.
 Figure 1: (A) Abdominal radiography shows a linear calcified body in the right abdomen (arrow). (B) Abdominal ultrasonography shows intestinal echo in the right mid-clavicular line in the abdominal cavity at the level of the umbilical horizontal line (arrow). (C) Abdominal MRI scan shows a linear, dense foreign body wrapped by greater omentum (arrow).
Figure 1: (A) Abdominal radiography shows a linear calcified body in the right abdomen (arrow). (B) Abdominal ultrasonography shows intestinal echo in the right mid-clavicular line in the abdominal cavity at the level of the umbilical horizontal line (arrow). (C) Abdominal MRI scan shows a linear, dense foreign body wrapped by greater omentum (arrow).
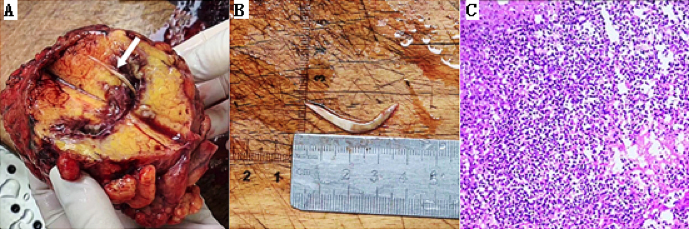 Figure 2: (A) A fishbone found embedded (arrow) in the greater omentum. (B) On gross examination, the foreign object was identified as a 3.5 cm long fishbone. (C) Histopathology reveals acute inflammatory lesion in the greater omentum (H&E; 40).
Figure 2: (A) A fishbone found embedded (arrow) in the greater omentum. (B) On gross examination, the foreign object was identified as a 3.5 cm long fishbone. (C) Histopathology reveals acute inflammatory lesion in the greater omentum (H&E; 40).
DISCUSSION
Foreign body ingestion by gastrointestinal route is a very common occurrence that needs urgent diagnosis and adequate treatment. Fishbone is one of the most common foreign bodies ingested into our bodies.4 While most ingested foreign bodies (80%-90%) pass through the gastrointestinal tract without any complication, probably 10% to 20% of foreign bodies need to be removed by endoscopy, and less than 1% perforate and need surgery.5
In this case, we report an ingested fishbone not passing smoothly through but penetrating gastrointestinal tract and causing granulomatous inflammation of the greater omentum with local suppuration. The reason for the delayed treatment of the patient was the neglect of minor symptoms by the patient. According to the history of fishbone intake and the MRI findings, we were able to make an accurate diagnosis of fishbone penetrating the stomach wall before the operation. Firstly, we attempted to remove the foreign object by the endoscope but failed because it was not found. Subsequently, an emergency exploratory laparotomy was carried out. The foreign body was removed successfully and safely by laparotomy, and was identified as a 3.5 cm long fishbone. Histopathological findings revealed an inflammatory response around the fishbone piercing the greater omentum.
Despite the fact that most accidentally ingested fishbones migrate distally inside the lumen, they may also remain embedded within the thick gastric wall, migrate to other parts of the body, perforate, and may result in abscess or granuloma formation. We retrieved the PubMed database for case reports of ingested fishbones in the English language from January 1970 to March 2019. The retrieval results included more than 200 articles. We found that the ingested fishbones can migrate to many parts of the body, besides digestive tract perforation,6,7 such as the thyroid gland, soft tissues of the neck, superior mediastinum, aorta, left atrium, common carotid artery, internal jugular vein, pancreas, bile ducts, and liver.8-10 But it is exceedingly rare that the fishbone penetrates through the stomach wall, pierces the greater omentum, and results in granulomatous inflammation. In the present case, the fishbone was embedded in the greater omentum and was removed successfully and safely by laparotomy.
In summary, this case demonstrates that an ingested fishbone can cause granulomatous inflammation of the greater omentum with local suppuration, and also indicates that timely imaging examination is important for timely diagnosis and management.
ACKNOWLEDGEMENT:
This project is funded/supported by the joint fund project of Hubei Provincial Health Committee (WJ2019H510) and Yichang Social Science Fund (ysk17kt231).
PATIENT’S CONSENT:
Informed consent was obtained from the patient for publishing his details and data.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
TF: Concept, data collection and interpretation, literature search, and manuscript writing.
CQW: Concept, data collection, literature search, manuscript preparation, and editing.
SYJ: Laparotomy operator, data acquisition, data analysis, and manuscript preparation.
WYW: Design, definition, and intellectual content.
YNW: Concept, design, definition, and intellectual content.
XTL: Concept, data collection, and interpretation.
REFERENCES
- Guelfguat M, Kaplinskiy V, Reddy SH, DiPoce J. Clinical guidelines for imaging and reporting ingested foreign bodies. AJR Am J Roentgenol 2014; 203(1):37-53. doi: 10.2214/AJR.13.12185.
- Jain A, Nag HH, Goel N, Gupta N, Agarwal AK. Laparoscopic removal of a needle from the pancreas. J Minim Access Surg 2013; 9(2):80-1. doi: 10.4103/0972-9941.110968.
- Michael B, Peter B, Pierre DH, Michael H, Dirk H, Cesare H, et al. Removal of foreign bodies in the upper gastrointestinal tract in adults: European society of gastrointestinal endoscopy (ESGE) clinical guideline. Endoscopy 2016; 48(5):489-96. doi: 10.1055/s-0042- 100456.
- Kim HU. Oroesophageal fishbone foreign body. Clin Endosc 2016; 49(4):318-26. doi: 10.5946/ce.2016.087.
- Rui X, Bi-Guang T, Hui-Chao W. Unexplained abdominal pain due to a fishbone penetrating the gastric antrum and migrating into the neck of the pancreas: A case report. World J Clin Cases 2019; 7(6):805-8. doi: 10.12998/wjcc.v7.i6.805.
- Ahmet Cem D, Muhammet Ferhat C, Hakan Y, Cevher A, Mahmut D, Halil A. Laparoscopic resection and intracorporeal anastomosis of perforated small bowel caused by fishbone ingestion. Ulus Travma Acil Cerrahi Derg 2016; 22(6):572-4. doi: 10.5505/tjtes.2016.88137.
- Congcheng F, Liping Y, Xinli M, Jinshun Z. Endoscopic treatment of a sigmoid perforation caused by an ingested fishbone. Endoscopy 2017; 49(S01):E82-E3. doi: 10.1055/s-0042-124500.
- Ya Ling T, Ting Ting Q, Jia X, Nai Yun C, Mei Fang Y. Successful treatment of an acute infective endocarditis secondary to fishbone penetrating into left atrium caused by Granulicatella adiacens and Candida albicans. Medicine (Baltimore) 2017; 96(51):9185. doi: 10.1097/ MD.0000000000009185.
- Husna JH, Bee-Lian K, Zulkifli Y, Irfan M. Migrating fishbone piercing the common carotid artery, thyroid gland and causing deep neck abscess. World J Clin Cases 2016; 4(11):375-9. doi: 10.12998/wjcc.v4.i11.375
- Masaaki A, Masashi K, Mizuho M, Ichiro S, Mariko T, Junichi K, et al. Fishbone migration to bile ducts after pancreaticoduodenectomy: A case series. Abdom Radiol (NY) 2019; 44(4):1217-22. doi: 10.1007/s00261- 018-1875-7.