Giant Sigmoidal Lipoma Protruding Through Anal Canal and Causing Sigmoido-rectal Intussusception
By Ali Surmelioglu1, Serhat Ozer2Affiliations
doi: 10.29271/jcpsp.2022.08.S118ABSTRACT
Intussusception is a rare condition in adulthood and there exists an underlying pathological lesion in most cases. Colorectal lipoma is the second most common benign tumour of the colon. Although commonly asymptomatic, it can present with intussusception. We, herein, report a case of a 79-year female with a yellowish mass with irregular surface prolapsing through the anal canal. In computed tomography (CT), sigmoido-rectal intussusception plus a lesion with the regular borders originating from the distal sigmoid colon protruding through the anal canal were observed. We resected the lesion with a transanal approach, following which the intussusception resolved spontaneously. Histopathological examination had reported lipoma. Transanal resection is a safe and efficient method of the treatment in distal colorectal lipomas presenting with intussusception.
Key Words: Colorectal lipoma, Sigmoido-rectal intussusception, Transanal resection.
INTRODUCTION
Colorectal lipomas are usually asymptomatic benign and solitary tumours originating from the submucosal connective tissue of the bowel wall that is located mostly in the ascending colon.1,2 Giant lipomas defined as larger than 4 cm, tend to be symptomatic, and may present with rectal bleeding, abdominal pain, or alterations in the bowel movements.1 Rarely, these may present with intussusception. Moreover, it is extremely rare for the distally located lipomas to cause sigmoido-rectal intussusception and protrude through the anal canal.3,4 Herein, the diagnosis and treatment of an elderly female patient with a giant lipoma protruding through anal canal leading to sigmoido-rectal intussusception are presented.
CASE REPORT
A 79-year woman presented to our emergency room with the abdominal pain and palpable mass protruding from the anus. In her medical history, the patient described abdominal pain for 6 months along with a palpable mass protruding out of the anus occasionally. On physical examination, nothing was notable except the minimal abdominal tenderness.
Perianal examination revealed a yellowish soft tissue mass measuring 5×5 cm with the regular borders and a rough surface which was found to have a thick peduncle after traction (Figure 1a). The mass could not be reduced therefore, with digital help, rectosigmoidoscopy was performed and malignancy was ruled out. On CT scan of abdomen and pelvis, a soft tissue mass with regular borders originating from the distal sigmoidal region and protruding through the anal canal causing sigmoido-rectal intussusception (target sign) was observed (Figure 1b). No additional test was taken. The origin was approached by traction of the mass in the lithotomy position under general anaesthesia (Figure 2a). The mass was totally excised transanally using linear cutter (Figure 2b). The patient was discharged on the second postoperative day, while intussusception did not resolve in the early postoperative period. Patient had no complaint and rectosigmoidoscopy revealed resolved intussusception on day 10. In histopathological examination, a submucosal lipoma with 5.3×5.5 cm diameter was reported.
DISCUSSION
Colorectal lipoma is the second most common benign tumour of the colon (0.035-4.4%) following adenomatous polyps.2 It was first described by Bauer in 1757.5 It usually originates from mature adipocytes in submucosal connective tissue of the intestinal wall. The chronic irritation and inflammation are thought to be responsible for excessive fat tissue accumulation.6 Colorectal lipoma is more commonly seen in women aged 50-65 years. It is usually found incidentally as solitary, well delineated, and sessile mass in colonoscopy.
 Figure 1a: Soft tissue mass lesion protruding from the anus.
Figure 1a: Soft tissue mass lesion protruding from the anus.
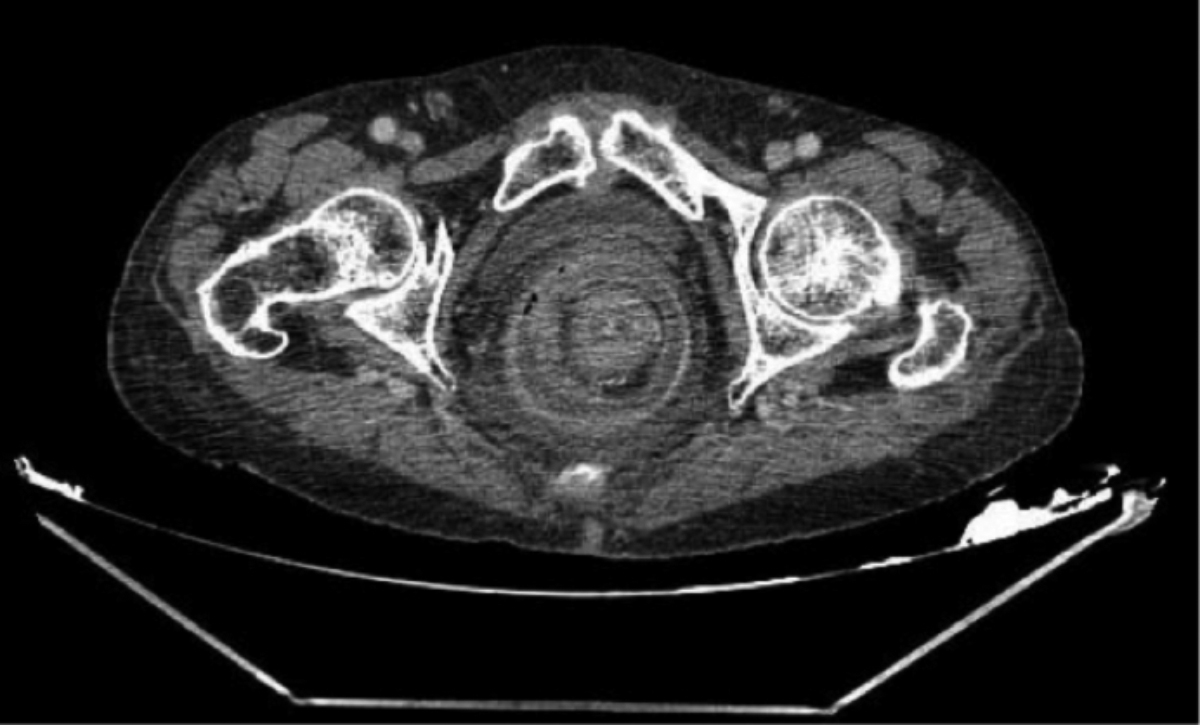 Figure 1b: Target sign image in contrast-enhanced axial pelvic CT scan caused by the intraluminal soft tissue mass (lipoma) leading to intussusception.
Figure 1b: Target sign image in contrast-enhanced axial pelvic CT scan caused by the intraluminal soft tissue mass (lipoma) leading to intussusception.
It can be multiple in the cecum (10-20%). It is are most frequently localised in the ascending colon (61%) followed by descending colon (20.1%), transverse colon (15.4%), and the rectum (3.4%).2,6
Three types of lipoma have been defined: submucosal (composing 90% of the cases), subserosal, and mixed. In macroscopic appearance, they are seen as round, yellowish, and sessile or pedunculated masses with the smooth or rough surfaces while microscopy reveals lobulated adipose tissue accumulation surrounded by a fibrous capsule. Risk of malignant transformation is extremely low. Colorectal lipomas are usually asymptomatic (94%) and incidentally found during colonoscopy, surgery or autopsy.1,6 Size is the predictor of symptoms i.e. lesions larger than 2 cm tend to be symptomatic. Those between 2-3 cm are symptomatic in 30% of the cases.7 If they are larger than 4 cm, they are called “giant” lipomas and are symptomatic in 75% of cases.1,7
As for symptoms, abdominal pain (42.4%), rectal bleeding (54.5%), and altered bowel movements (24.2%) are mostly encountered.1,7 Other reported symptoms with the lower frequency include constipation, obstruction, intussusception, and anaemia.1,2 In some cases, ulceration, granulation, or fat necrosis can develop at the wall layer underlying the lesion leading to the self-amputation and spontaneous expulsion.1,7
 Figure 2a: The stalk of large pedunculated lipoma before transanal resection.
Figure 2a: The stalk of large pedunculated lipoma before transanal resection.
 Figure 2b: Transanal resection of the lesion with the help of linear cutter.
Figure 2b: Transanal resection of the lesion with the help of linear cutter.
Intussusception is a rare disorder in adulthood, which comprises 1-3% of all the intestinal obstructions.8 In contrast to the childhood cases, there is a pathologic lesion as a lead point in 90% of the adult intussusception cases. Abdominal CT has diagnostic value in 58-100% of the cases.7,8 The typical finding is a target sign or sausage-shaped mass caused by the soft tissue lesion causing intussusception. While small bowel intussusception is secondary to benign lesions in 70% of the cases, large bowel intussusception is malignancy-related in 60-65% of the cases.8 As described in this case, one of the rare benign causes of adulthood colorectal intussusception is colorectal lipoma, rectal prolapse, colonic malignancy, and gastrointestinal stromal tumour should be considered in the differential diagnosis.
Follow-up is recommended in asymptomatic small lesions; however, in symptomatic cases, endoscopic or surgical treatment should be considered. The treatment modality is based on localisation, risk of malignancy, and complications. The endoscopic resection is appropriate in symptomatic lesions less than 2 cm in size.1,7 However, due to the recent advances, even larger lesions can be resected via endoscopy. In case of large sessile lesions, malignancy, massive haemorrhage, or obstruction, surgical approach should be considered. Colotomy plus lipectomy should be the primary method in the uncomplicated cases with known preoperative diagnosis. Segmental colon resection can be applied when needed. Larger resections, such as hemicolectomy, can be performed in case of the complications or suspicion of malignancy. Unfortunately, owing to the lack of preoperative diagnosis in majority of the cases, the rate of unnecessary laparotomy and large resection is not low. Reduction and lipectomy or segmental resection can be performed in the colocolic intussusception cases with no diagnostic suspicion. However, since the majority of the adulthood intussusception cases are malignancy-related, radical colectomy is usually done. Laparoscopy should be preferred since it is associated with the less pain, shorter hospital stay, and fast recovery. Exact localisation can be tough to detect during laparoscopic approach in some cases, which can be overcome by preoperative endoscopic marking or intraoperative colonoscopy. Surgery is an efficient way of the treatment and no recurrence has been reported to date.1,7,8
Few cases of sigmoidal lipoma leading to the intussusception have been reported in the literature. Mohamed et al. performed sigmoidal resection plus end colostomy in a case presented with the sigmoido-rectal intussusception.9 Ferzaneh et al. applied transanal resection in a rectal lipoma-related colorectal intussusception case three weeks after barium enema reduction.10 The cases of spontaneous lipoma expulsion and transanally resected lipoma prolapsing through the anus have been reported in the literature.1,7 Two cases of giant sigmoidal lipoma leading to both sigmoido-rectal intussusception and anal protrusion have been reported to date. Of these, one was treated with laparotomy, reduction, colostomy, and lipectomy while the other with laparotomy plus sigmoidal colon resection.3,4 In the present case, we performed transanal resection, and intussusception resolved spontaneously during the follow-up. Transanal simple resection is the safe and reliable treatment method in benign lesions leading to intussusception originating from rectosigmoid junction.
PATIENT’S CONSENT:
Informed consent was obtained for this case report.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
AS: Conception and design.
SO: Critical Revision and final approval.
All the authors have approved the final version of the manuscript to be published.
REFERENCES
- Omar MG, Julia S, Puneet S, Richard FH, Joseph DD. Pedunculated colonic lipoma prolapsing through the anus. World J Clin Cases 2015; 3(5):457-561. doi: 10.12998/wjcc. v3.i5.457.
- Jiang L, Jiang LS, Li FY, Ye H, Li N, Cheng NS, et al. Giant submucosal lipoma located in the descending colon: A case report and review of the literature. World J Gastroenterol 2007; 13(42):5664-7. doi: 10.3748/wjg.v13.i42.5664.
- West CT, Pilarski A, White D, Ricketts D. An intussuscepting colonic lipoma causing prolapse of the sigmoid colon in an adult. Br J Hosp Med 2019; 80(3). doi: 10.12968/hmed. 2019.80.3.ii.
- Elliott M, Martin J, Mullan F. Prolapsed giant sigmoid lipoma: A rare cause of adult ischaemic intussusception. BMJ Case Rep 2014. doi:10.1136/bcr-2014-204036.
- Ryan J, Martin JE, Pollock DJ. Fatty tumours of the large intestine: A clinicopathological review of 13 cases. Br J Surg 1989; 76(8):793-6. doi: 10.1002/bjs.1800760809.
- Ghidirim G, Mishin I, Gutsu E, Gagauz I, Danch A, Russu S. Giant submucosal lipoma of the cecum: Report of a case and review of literature. Rom J Gastroenterol 2005; 14(4): 393-6.
- Kouritas VK, Baloyiannis I, Koukoulis G, Mamaloudis I, Zacharoulis D, Efthimiou M. Spontaneous expulsion from rectum: A rare presentation of intestinal lipomas. World J Emerg Surg 2011; 6:19. doi: 10.1186/1749-7922-6-19.
- Yakan S. Intussusception in adults: Clinical characteristics, diagnosis and operative strategies. World J Gastroenterol 2009; 15(16):1985. doi: 10.3748/wjg.15.1985.
- Mohamed M, Karim E, Donald S, Kenneth W, Michael M. Adult sigmoidorectal intussusception related to colonic lipoma: A rare case report with an atypical presentation. Int J Sur Case Reports 2015; 10:134-7. doi: 10.1016/j.ijscr. 2015.03.035.
- Farzaneh S, Mersad M, Hossein S. Rectal lipoma as a lead point for colo-colonic intussusception. Radiol Case Rep 2018; 13(2):431-3. doi: 10.1016/j.radcr.2018.01.012.