Broad Complex Tachycardia, Addison's disease, and Ascending Flacid Paralysis: An Interesting Case on Cardiology Floor
By Nauman AliAffiliations
doi: 10.29271/jcpsp.2022.08.S98ABSTRACT
Broad complex tachycardia is a common presentation in the cardiology emergency room but is not always due to ventricular tachycardia, especially in a young patient who has other important medical illnesses and with no underlying cardiac illness. We present a case of a 40-year male who was admitted with complaints of palpitation associated with rapidly progressive weakness of lower limbs progressing to quadriparesis in about 10 hours. His clinical presentation was due to hyperkalemia and weakness due to Addison's disease. The patient was treated with drugs to lower potassium levels and steroids. His muscle power improved dramatically as potassium levels normalized and he recovered completely.
Key Words: Acute flaccid paralysis, Hyperkalemia, Broad complex tachycardia.
INTRODUCTION
Broad complex regular tachycardia (BCRT) is usually treated as ventricular tachycardia (VT) in cardiology emergencies when the physician is unable to differentiate among different causes of BCRT. Sometimes the underlying cause of BCRT mimicking VT may be a rare disease that requires a high degree of suspicion. This is especially pertinent when the patient has some underlying medical illness that can cause ECG changes simulating VT. Hyperkalemic ECG changes are one of such abnormalities. Hyperkalemia can also cause rapidly progressing ascending paralysis. Hyperkalemia can occur from many diseases including kidney failure, medicines that can increase potassium levels, and Addison's disease (AD), etc.1 We describe one such case of a young male patient of AD presenting with palpitations and ascending pattern of paralysis of limbs. His ECG showed BCRT. He was initially treated as a case of VT. He was hyperkalemic due to untreated AD. Clinical suspicion, diagnosis, and treatment of our case led to prompt recovery and resolution of ECG changes.
CASE REPORT
A 40-year male was admitted in the cardiology emergency room (ER) with complaints of generalized weakness, a history of syncope, and dyspnoea. His past medical record was reviewed and showed that he was diagnosed with AD 17 years ago and Guillain-Barre Syndrome (GBS) one year ago. He was diagnosed with complaints of generalized weakness and since then he is on replacement therapy of prednisolone and fludrocortisone. About one year ago, he presented in the neurology clinic with complaints of body weakness and was diagnosed as a case of GBS as his weakness was more in the lower limbs. He was areflexic and nerve conduction studies suggested acute demyelinating sensory-motor polyneuropathy (Figure 1). However, his cerebrospinal fluid (CSF) examination did not show protein cell dissociation at that time, which is a hallmark of GBS. Five sessions of plasmapheresis were done for treatment of GBS and the patient recovered in 3 weeks. About four months ago, he again developed similar weakness and was diagnosed as case of recurrent GBS. He was tested and treated on the same lines with recovery in 2 weeks. His current visit in ER was with syncope, dyspnea, and generalized weakness, more in the lower limbs. His ECG showed BCRT and a suspicion of venVT as shown in Figure 2. The cardiology team was consulted and the patient was shifted to Cardiac Unit considering VT as the dominant clinical parameter, where initial treatment was started with amiodarone for VT while blood chemistry reports were awaited. Neurological consultation was taken and they considered a weakness to be possibly due to the third recurrence of GBS in a year considering past history, weakness, areflexia, and results of nerve conduction study. A careful second review of ECG and clinical history made us to revise our initial diagnosis. Taking together BCRT and acute flaccid paralysis in a patient with AD raised a strong possibility that both could be due to hyperkalemia. Serum potassium was 7.8 mmol/l and sodium was 119 mmol/l. The potassium level was corrected by glucose/insulin infusion. Injection of calcium gluconate was also given as cardioprotective membrane stabiliser.
He was also given intravenous hydrocortisone, 100 mg, three times a day and 0.9% sodium chloride, 50 ml/hour. The patient had a full recovery from weakness in 2 days as his potassium and sodium levels were normalised. The ECG also reverted to normal sinus rhythm (Figure3).
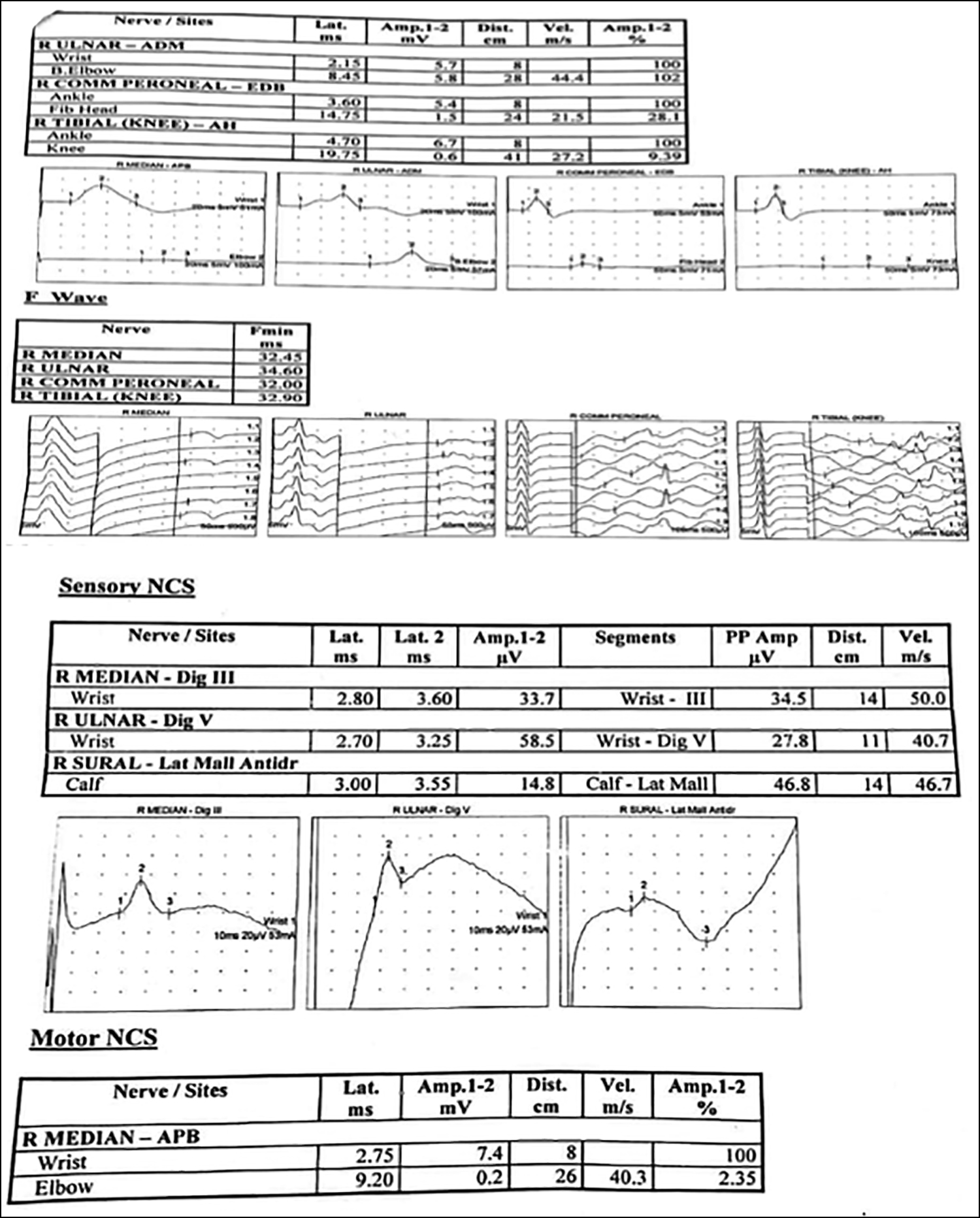 Figure 1: Nerve conduction studies showing acute demyelinating polyneuropathy.
Figure 1: Nerve conduction studies showing acute demyelinating polyneuropathy.
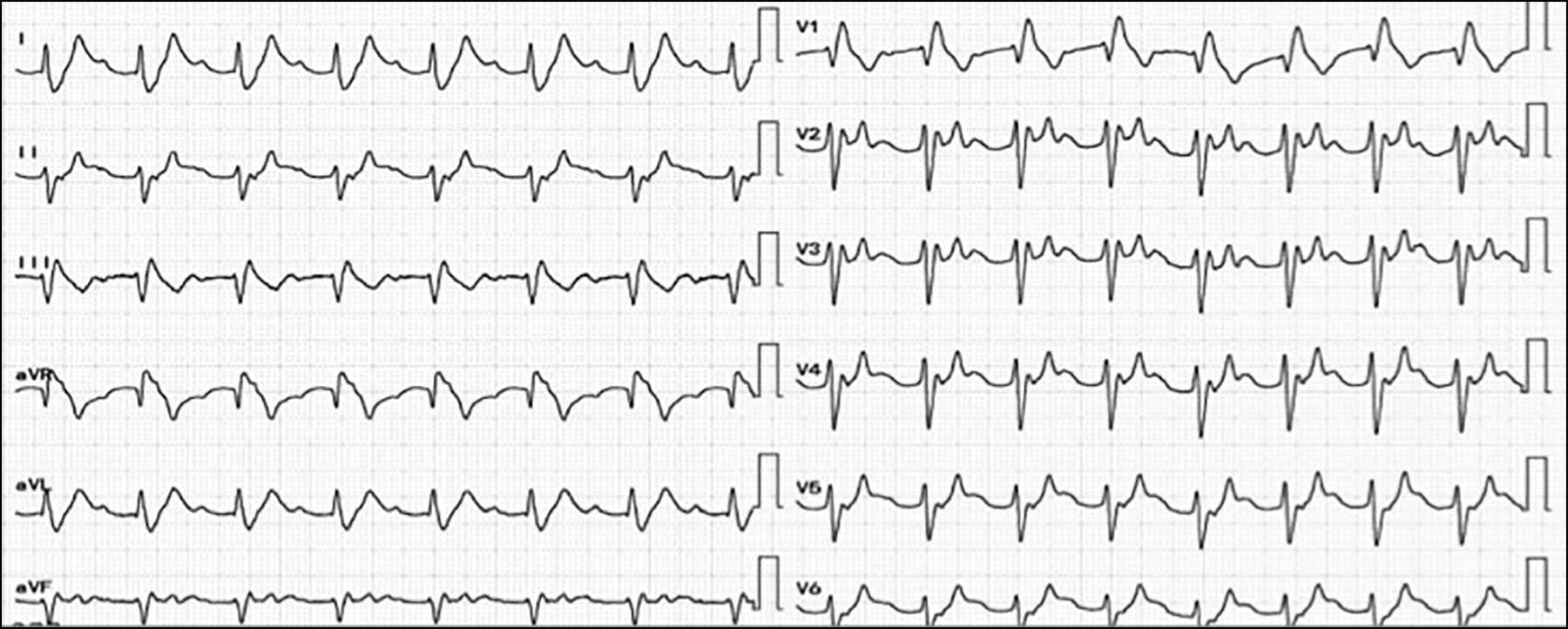 Figure 2: Initial ECG of the patient, showing broad complex regular tachycardia.
Figure 2: Initial ECG of the patient, showing broad complex regular tachycardia.
DISCUSSION
Hyperkalemia is labeled when serum level is >5.5 mEq/L. Pathophysiologically, it is due to the membrane conduction problems. The consequent cardiac problems are dangerous and include cardiac rhythm disorders. All can manifest with a series of ECG changes as the potassium level progressively rises. With a potassium level of >7 mEq/L, ECG changes can mimic VT as BCRT with no visible p waves. Other symptoms include diseases at muscle conduction level, respiratory paralysis, etc. This case was different because he presented with syncope and paralysis of all four limbs in ascending order. His past clinical history was significant for AD (Figure 4) and recurrent GBS.
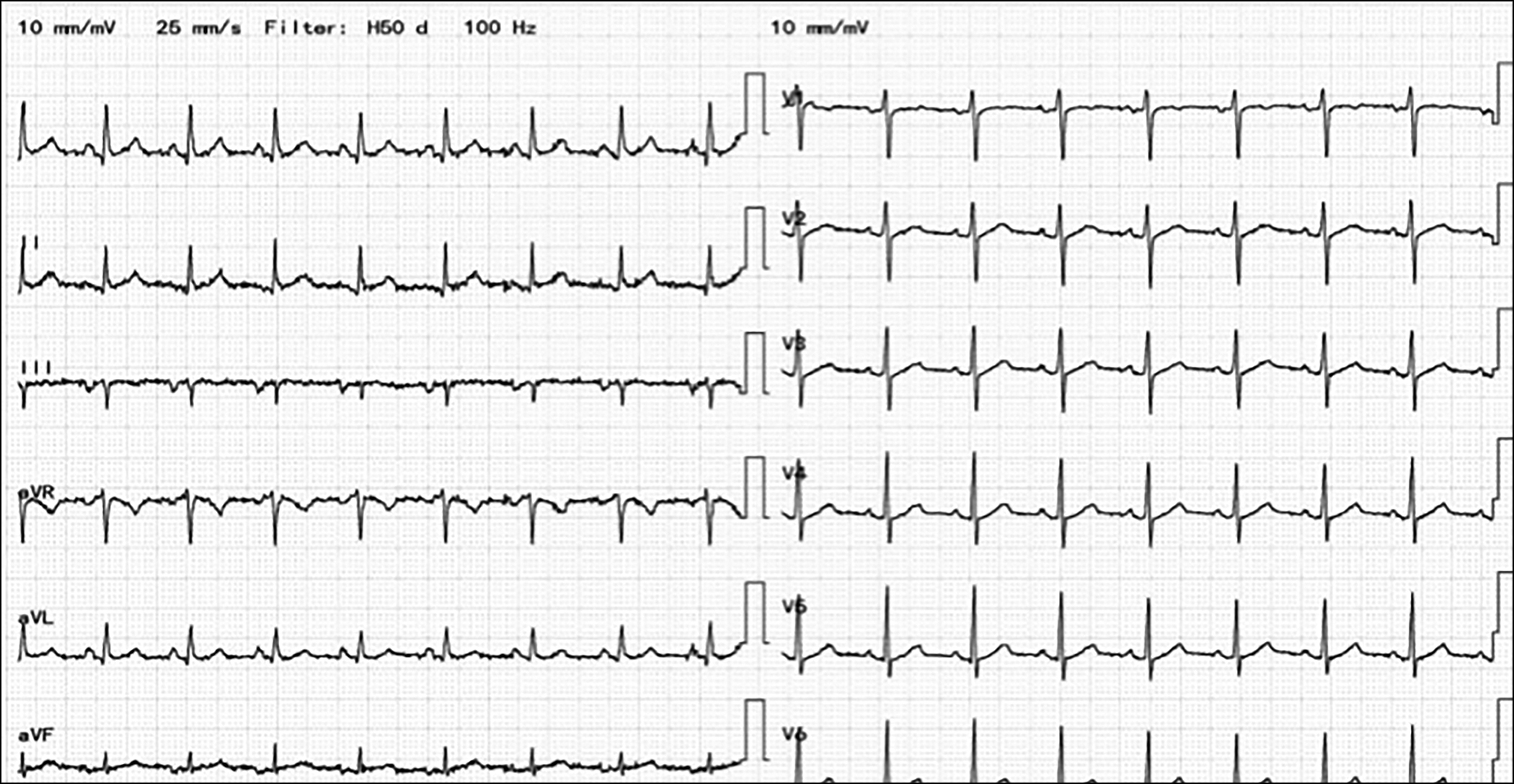 Figure 3: Normal ECG, after normalisation of potassium levels.
Figure 3: Normal ECG, after normalisation of potassium levels.
 Figure 4: Pigmentation on the face of the patient due to raised ACTH hormone level due to Addison's disease.
Figure 4: Pigmentation on the face of the patient due to raised ACTH hormone level due to Addison's disease.
Quadriparesis induced by hyperkalemia is described as hyperkalemic periodic paralysis (HPP) which can be primary or secondary HPP.1-6 Acute flaccid paralysis can simulate GBS but that difference is that GBS has an only motor weakness.7 Contrary to this disturbance related to autonomic nervous system found in GBS and is not a clinical feature of paralysis associated with high potassium levels.8 Weakness due to high potassium level is probably due to effects at cellular conduction level.9,10
A review of the literature revealed several case reports of HPP associated with adrenal insufficiency. In their study, Sowden and Borsey have reported HPP as an initial symptomatic manifestation of AD in a patient with diabetes mellitus.11 Hyperkalemic paralysis in established cases is attributed to inadequate steroid replacement or excess administration of potassium supplements.12
As in this patient, reversal of paralysis started almost immediately after lowering potassium level, with full power returning over the next few hours.
Normalisation of ECG as potassium level was corrected confirms that this patient was having hyperkalemic ECG manifestation. With his rapid and complete recovery and also the fact that three recurrences of GBS in a year are very rare, we consider this as a case of secondary HPP due to underlying AD. Nerve conduction study findings are very similar in both GBS and HPP and sometimes can be misleading. However, their rapid resolution is also a feature of HPP and not of GBS.
To conclude, hyperkalemia may be a potentially life-threatening but rapidly reversible cause of quadriparesis and cardiac arrhythmias. A strong index of suspicion should be the key to early diagnosis in a patient with a potential underlying causes like AD.
PATIENT’S CONSENT:
Informed consent was taken from the patient to publish his data.
COMPETING INTEREST:
The author declared no competing interest.
AUTHOR'S CONTRIBUTION:
NA: Conceived the idea, collected data, and wrote different sections of the case report.
REFERENCES
- Naik KR, Saroja AO, Khanpet MS. Reversible electro-physiological abnormalities in acute secondary hyperkalemic paralysis. Ann Indian Acad Neurol 2012; 15(4):339-43. doi: 10.4103/0972- 2327.104354.
- Kumar KS, Ramakrishna C, Padmanabhan S, Kumar VS. Hyperkalemic quadriparesis in a patient of ESRD. Indian J Nephrol 2005; 15(3):108-9.
- Desport E, Leroy J, Nanadoumgar H, Chatellier D, Robert R. An unusual diagnostic of quadriparesia: Hyperkalemic paralysis. Report of four non-familial cases. Rev Med Interne 2006; 27(2):148-51. doi: 10.1016/j.revmed. 2005.10.008.
- Berrebi R, Orban JC, Levraut J, Grimaud D, Ichai C. Secondary hyperkalaemic acute flaccid tetraplegia. Ann Fr Anesth Reanim 2009; 28(4):381-3. doi: 10.1016/j. annfar.2009.02.014.
- Wahab A, Panwar RB, Ola V, Alvi S. Acute onset quadriparesis with sine wave: A rare presentation. Am J Emerg Med 2011; 29(5):575.e1-2. doi: 10. 1016/j.ajem. 2010.05.021.
- Panichpisal K, Gandhi S, Nugent K, Anziska Y. Acute quadriplegia from hyperkalemia: A case report and literature review. Neurologist 2010; 16(6):390-3. doi: 10.1097/NRL.0b013e3181b120b8.
- Evers S, Engelien A, Karsch V, Hund M. Secondary hyperkalaemic paralysis. J Neurol Neurosurg Psychiatry 1998; 64(2):249-52. doi: 10.1136/jnnp. 64.2.249.
- Perez GO, Oster JR, Pelleya R, Caralis PV, Kem DC. Hyperkalemia from single small oral doses of potassium chloride. Nephron 1984; 36(4):270-1. doi: 10.1159/0001 83167.
- Livingstone IR, Cumming WJ. Hyperkalaemic paralysis resembling Guillain-Barré syndrome. Lancet 1979; 2(8149):963-4. doi: 10.1016/s0140- 6736(79)92663-1.
- Villabona C, Rodriguez P, Joven J, Costa P, Avila J, Valdes M. Potassium disturbances as a cause of metabolic neuromyopathy. Intensive Care Med 1987; 13(3): 208-10. doi: 10.1007/BF00254706.
- Sowden JM, Borsey DQ. Hyperkalaemic periodic paralysis: A rare presentation of Addison's disease. Postgrad Med J 1989; 65(762):238-40. doi: 10.1136/ pgmj.65.762.238.
- Faw ML, Ewer RW. Intermittent paralysis and chronic adrenal insufficiency. Ann Intern Med 1962; 57: 461-3. doi: 10.7326/0003-4819-57-3-461.