Neglected Heterotopic Interstitial Pregnancy
By Jingjing Feng, He Dan Wang, Wen LvAffiliations
doi: 10.29271/jcpsp.2020.12.1360Sir,
Heterotopic interstitial pregnancy is considered a rare form of ectopic pregnancy, which is not clearly defined as yet. In USA, the incidence of heterotopic interstitial pregnancy has risen from 1% to 3% due to in-vitro fertilisation (IVF) and embryo transfer (ET) in recent years;1 but this is not common in Pakistan. Heterotopic interstitial pregnancy stems from both abnormal embryo transport and the changes of tubal environment. Among the possible risk factors, smoking and infection have been shown to decrease ciliary beat frequency, which will affect the ovum transport and fertility. Secondly, estradiol (E2) and nitric oxide (NO) are associated with increased ciliary motility. NO has an effect on the smooth muscle of fallopian tube, and E2 may be involved in gene regulation and expression. Finally, inflammation can lead to the damage of tubal structure with consequent tubal dysfunction, and ultimately, retention of an oocyte or embryo. All of these factors can affect embryo implantation.2,3
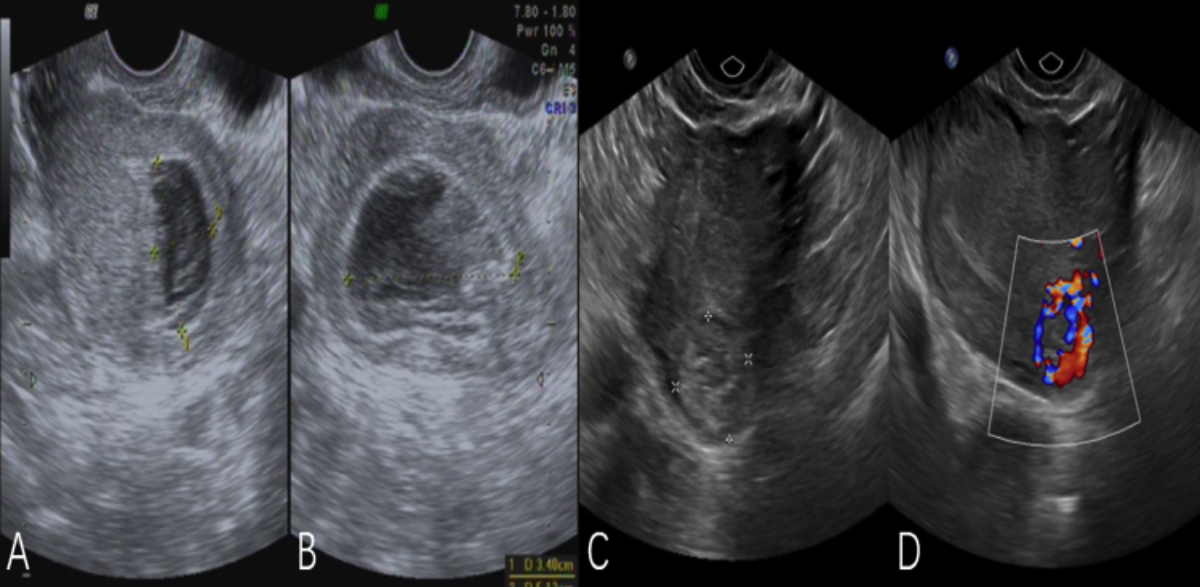 Figure 1 (A, B): Pre-uterine curettage ultrasound. (C, D): Ultrasound repeated after uterine curettage.
Figure 1 (A, B): Pre-uterine curettage ultrasound. (C, D): Ultrasound repeated after uterine curettage.
 Figure 2: Laparoscopic view of the uterine cornua and left fallopian tube.
Figure 2: Laparoscopic view of the uterine cornua and left fallopian tube.
A 36-year female, gravida 3, para 1 (G3P1), presented to gynecologic clinic with menolipsis for 50 days and vaginal bleeding twice. A transvaginal ultrasound was performed which showed a 5.1×3.4×1.8 cm uneven echogenic mass and uterine myoma (Figure 1 AB). Next day, under direct vision by ultrasound, uterine curettage was performed. On second day after surgery, compared to preoperation, the serum β-HCG was found higher. An emergency ultrasound examination revealed medium to high, in-homogeneous echogenic mass located in the left cornua uteri and uterine myoma (Figure 1 CD). Laparoscopic exploration was performed. The left uterine cornua was obviously raised and the size of this mass was 4×4 cm with prominent vascularity on the surface. The left fallopian tube appeared slightly distorted (Figure 2). Finally, she underwent left salpingectomy as well as the removal of the left uterine cornua containing embryo. Serum β-HCG decreased significantly after operation. The pathology findings of uterine curettage showed placental villi and decidual tissue. The second surgery pathology showed heterotopic interstitial pregnancy.
Heterotopic interstitial pregnancy is extremely rare and poses diagnostic and treatment challenges and is frequently misdiagnosed. Careful evaluation of clinical symptoms, serology, and ultrasound is necessary for correct diagnosis of this disease. Diagnosis of heterotopic interstitial pregnancy by ultrasound requires careful examination. Gestational sac, fetal pole, cardiac activity, a hyperechoic circumferential ring called the bagel sign or blob sign can identify ectopic pregnancy.4 For patients with increased serum β-HCG after abortion, we should consider firstly, the common conditions such as incomplete abortion and ectopic pregnancy At the same time, we should be alarmed at the possibility of atypical heterotopic interstitial pregnancy and choriocarcinoma.5 Reviewing HCG and ultrasound after surgery may clarify the success of the uterine surgery; and in case, there is something unusual, it can be discovered and treated earlier.
CONFLICT OF INTEREST:
The authors declared no conflict of interest.
AUTHORS’ CONTRIBUTION:
JF, HDW: Responsible for the conception and design of the work, or revising it critically for important intellectual content.
WL: Final approval of the version to be published and agreed to be accountable for all aspects of the work.
REFERENCES
- Anderson J, Patterson C, Riley A. Heterotopic interstitial pregnancy: A case report. Case Rep in Women's Health 2018; 17:8-10. doi: 10.1016/j.crwh.2018.02.003.
- Shaw JL, Dey SK, Critchley HO, Horne AW. Current knowledge of the
aetiology of human tubal ectopic pregnancy. Hum Reprod Update 2010; 16(4):432-44. doi: 10.1093/humupd/dmp057. - Magers T, Talbot P, DiCarlantonio G, Knoll M, Demers D, Tsai I, et al. Cigarette smoke inhalation affects the reproductive system of female hamsters. Reprod Toxicol 1995; 9(6):513-25. doi: 10.1016/0890-6238(95)02002-0.
- Panelli DM, Phillips CH, Brady PC. Incidence diagnosis and management of tubal and nontubal ectopic pregnancies: A review. Fertil Res Pract 2015, 1(1):15. doi: 10.1186/s40738-015-0008-z.
- Eom JM, Choi JS, Ko JH, Lee JH, Park SH, Hong JH, et al. Surgical and obstetric outcomes of laparoscopic management for women with heterotopic pregnancy. J Obstet Gynaecol Res 2013; 39(12):1580-6. doi: 10.1111/jog.12106.