Intercostal Nerve-based Neurilemmoma: Posing Diagnostic and Therapeutic Challenges
By Ibrahim Ethem Özsoy, Mehmet Akif TezcanAffiliations
doi: 10.29271/jcpsp.2020.08.886Sir,
Neurilemmomas, also called schwannomas/neurinomas, originating from Schwann cells in the nerve sheath, are benign, well-circumscribed, encapsulated, gray-brown colored, slow-growing neurogenic tumors.1,2 They are usually benign tumors, mostly asymptomatic and have a low potential for malignant transformation. They are usually located in the costovertebral sulcus within the thorax, and less than 10% originate from the intercostal nerves. In the studies, the SUVmax value of PET-CT for neurilemmomas was found to be in the range of 1.9-12; and in most cases, increased F18-fluorodeoxyglucose (FDG) uptake was detected. Therefore, PET-CT cannot help in accurate diagnosis in these patients.3 Because of the possibility of malignant transformation, they should be surgically removed when detected. They rarely recur when they are completely removed surgically.4,5
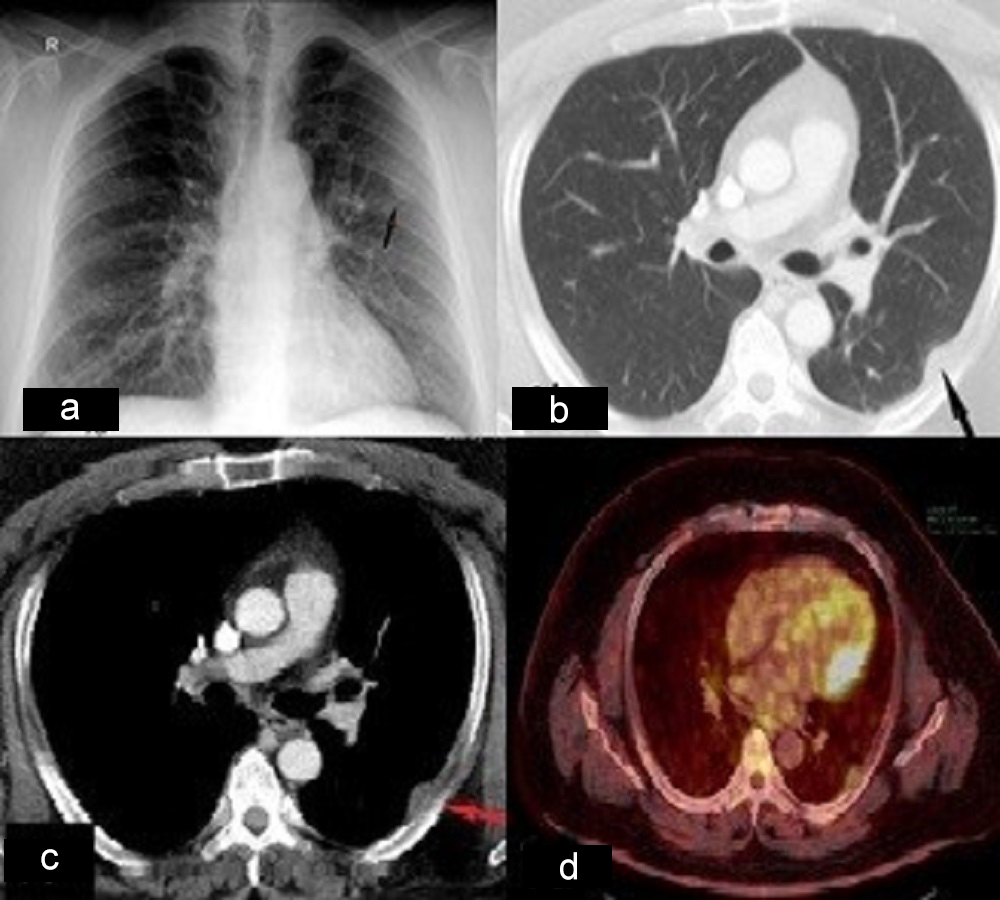 Figure 1: (a) An X-ray of the chest, revealed the left upper thoracic mass; (b, c) A chest tomography showing 14x23 mm sized tumor along the fourth rib (transaxial lung and mediastinal window CT images); (d) PET CT images show a mildly hypermetabolic mass lesion (SUVmax: 3.16) at the level of fourth rib.
Figure 1: (a) An X-ray of the chest, revealed the left upper thoracic mass; (b, c) A chest tomography showing 14x23 mm sized tumor along the fourth rib (transaxial lung and mediastinal window CT images); (d) PET CT images show a mildly hypermetabolic mass lesion (SUVmax: 3.16) at the level of fourth rib.
At the chest X-ray of a 47-year male admitted to a smoking cessation outpatient clinic with no respiratory symptoms, a suspicious hyperdensity in the left lung was seen (Figure 1a). His hemogram and biochemical laboratory values were normal. Physical examination revealed no pathology. Thoracic tomography (CT) scan showed nodular thickening in the left hemithorax, at the level of 4th rib, 14×23 mm sized, that was sitting on the pleura with a large base (Figures 1b, 1c). F-18 FDG PET-CT showed moderate hypermetabolism (SUVmax: 3.16) at the lesion site (Figure 1d). CT-guided transthoracic biopsy was planned, but could not be performed because the lesion was right next to the inner aspect of the rib. Because of the possibility of malignancy, it was decided to remove it surgically. On attempting to perform excision with videothoracoscopy, the thorax could not be entered, because of pleural adhesions, and round, well-circumscribed, encapsulated and soft lesion was excised through mini-thoracotomy (Figure 2). Histopathology and immunohistochemical examination revealed a spindle cell tumor with positivity of vessels for Factor VIII and CD34. The spindle cell component was strongly positive for S-100. A positivity rate of 1-2% was found with Ki-67 and a final diagnosis of neurilemmoma was made (Figure 3). The patient was discharged on the 3rd postoperative day.
 Figure 2: Round, well-circumscribed, encapsulated and soft lesion was excised.
Figure 2: Round, well-circumscribed, encapsulated and soft lesion was excised.
 Figure 3: (a) Cytoplasmic positive staining of spindle tumor cells with S-100 (x10); (b) Low proliferation with Ki-67 (x20).
Figure 3: (a) Cytoplasmic positive staining of spindle tumor cells with S-100 (x10); (b) Low proliferation with Ki-67 (x20).
In summary, increased F18-FDG uptake on PET-CT is found in almost all neurilemmomas, and PET-CT does not provide extra benefit. Surgical excision should be performed to make definitive histopathologic diagnosis and to exclude possible malignancy.
CONFLICT OF INTEREST:
No conflict of interest was declared by the authors.
AUTHORS’ CONTRIBUTION:
IEÖ: Data acquisition and analysis, interpretation, drafting, final approval.
MAT: Analysis and interpretation, drafting, final approval.
REFERENCES
- Reynolds M, Shields TW. Benign and malignant neurogenic tumours of mediastinum in children and adults. In: Shields TW, Locicero J, Reed Ce, Feins Rh, eds. General thoracic surgery, vol 2, 7th ed. Philadelphia: Lippincot Williams Wilkins 2009; 2415-39.
- Yapıcıer Ö, Ekemen S. Histopathology of schwannomas. Türk Nöroşir Derg 2016; 26(1):1-7.
- Benz MR, Czernin J, Dry SM, Tap WD, Allen-Auerbach MS, Elashoff D, et al. Quantitative f18-fluorodeoxyglucose positron emission tomography accurately characterizes peripheral nerve sheath tumors as malignant or benign. Cancer 2010; 116(2):451-8.
- McClenathan JH, Bloom RJ. Peripheral tumors of the intercostal nerves. Ann Thorac Surg 2004; 78(2): 713-4.
- Kransdorf MJ. Benign soft-tissue tumors in a large referral population: Distribution of specific diagnoses by age, sex, and location. AJR Am J Roentgenol 1995; 164(2):395-402.