Insight into COVID-19 Responses and Initiatives from Pakistan
By Salima Farooq1, Sonia Ijaz Haider2, Saima Sachwani1, Yasmin Nadeem Parpio1Affiliations
doi: 10.29271/jcpsp.2020.06.50ABSTRACT
The coronavirus pandemic is a rapidly evolving outbreak that has tremendously distressed people worldwide. The paper aims to present some key rapid responses and initiatives to COVID-19 undertaken in Pakistan. The information has been gathered by reviewing material and documents pertinent to COVID-19 in the context of Pakistan. The incidences of COVID-19 cases are gradually increasing; however, the case fatality rate is relatively lower in Pakistan as compared to developed countries. The government has taken massive actions, in terms of lockdowns, quarantine homes, testing facilities, closure of schools, and mass gatherings at places, to combat COVID-19. However, the measures seem to be insufficient due to the fear and stigma attached to it and the low socio-economic conditions. The government has launched initiatives, like Ehsaas cash dissemination programme, for the underprivileged families to address their basic needs; and philanthropic organisations are also coming forward to support these families. The spread of the pandemic is gradually increasing in Pakistan and we recommend strategies like increasing public awareness campaigns, improving screening capacity, and contact tracing to augment the efficiency of the current responses and initiatives.
Key Words: COVID-19, Pakistan, Responses, Initiatives.
The novel coronavirus disease, commonly known as COVID-19, is continuously putting unprecedented burden on the health and economic sectors worldwide. It was first identified in December 2019, in Wuhan, central China1. The virus has adversely affected people, irrespective of gender, socio-economic class, and geographical boundaries. The World Health Organization (WHO) officially declared the COVID-19 as a pandemic on March 11, 2020. As on April 20, 2020, this fast-growing pandemic, had infected 2,314, 621 people, with mortality of approximately 157,847 individuals, across the world2. The pandemic has not only substantially increased the risk of complications and mortality, but has also added to the psychological pressure and uncertainty; and affected socio-cultural dynamics. Moreover, this massive crisis has not only impacted developing countries, but the developed countries are also critically threatened and are gravely concerned about how to deal with its effects. This paper will shed light mainly on the responses and actions of the government of Pakistan, but also non-government organizations media, religious leaders, and the community at large, to combat this exponential outbreak.
To achieve the objective of the study, the authors reviewed and analysed media contents, including local and international reports, coverage in news channels, government updates, WHO assessments and guidelines, other related speeches and reports, and various websites, from January to April 21, 2020. Several countries have taken widespread measures to mitigate the effects of the disease; but not many countries seem to have realised the gravity of the situation after it was quite late. However, the government of Pakistan implemented numerous measures to limit the transmission of the disease even before the first case was reported (Figure 1). The result was that in Pakistan, the reported cases till April 21 were 9,565, with 201 deaths3. This figure may not depict the true picture, as many people in Pakistan are believed to be covering up the identification of this disease and the resultant deaths, due to fear of stigmatisation and isolation, and being kept away from their families at a time when they need them the most. According to the culture in Pakistan, not only the immediate family but also the extended family is expected to be around the patient for care and support. Moreover, as religious rites are an important part of burial, and the denial to perform these for corona-virus related deaths, is stopping people from declaring the disease and related deaths.
The country’s response to this critical situation included closing of international borders, and formulation of a COVID specific national action plan to guide preparedness and response to the current situation.
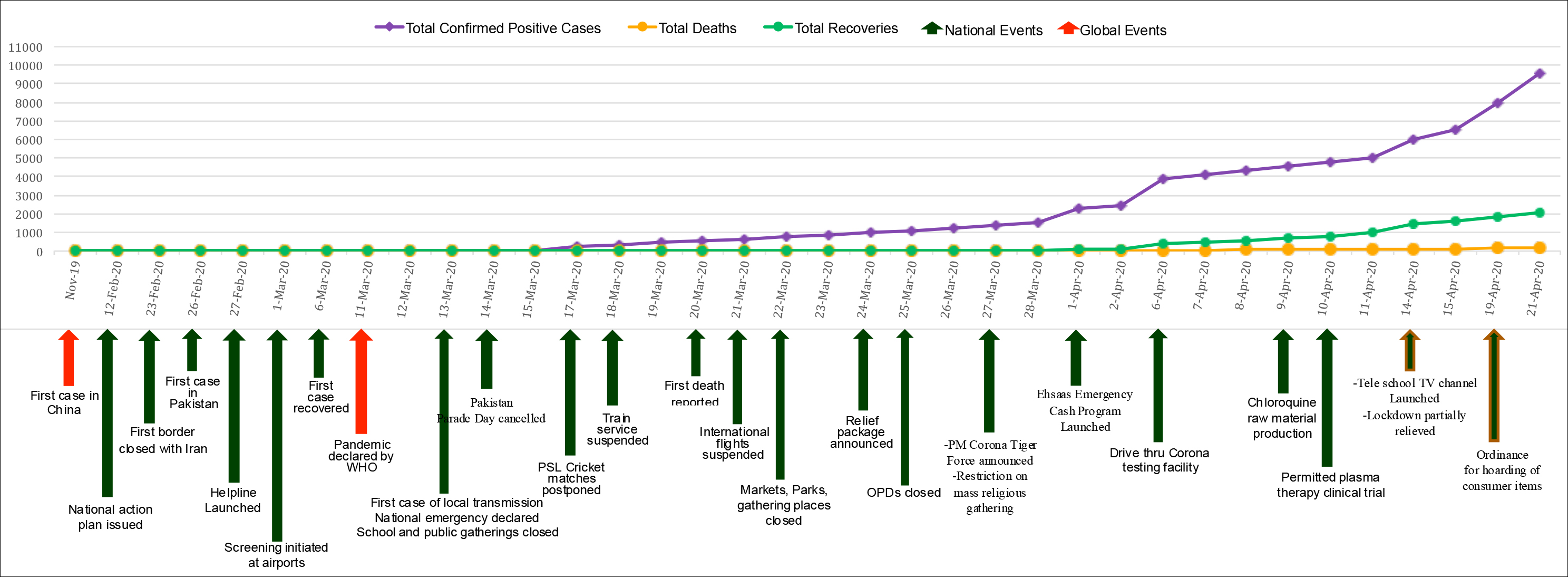 Figure 1: Series of events amid COVID-19 pandemic in Pakistan.
Figure 1: Series of events amid COVID-19 pandemic in Pakistan.
Besides this, very soon after the identification of the first case, on February 26, 2020, the government took further stringent actions, including suspension of international flights, cancellation of the Pakistan Super League cricket matches and the Pakistan Day celebrations (celebrated on March 23 each year, marking a significant day in Pakistan’s history). Moreover, a national emergency was declared, with lockdowns, quarantines, suspension of public transportation, closure of workplaces, schools, and outpatient services, and suspension of religious congregations.
In order to minimize the negative effects of the shutdown, the government initiated an emergency cash programme to meet the primary needs of about 12 million people who were likely to suffer the most. Another initiative of the government was the setting up of a volunteer, force, for which more than 1,000,000 volunteers have signed up. This centrally organised task force has been created to support the government in its initiatives, particularly if complete shutdown becomes imperative. These initiatives were needed as 45% of the Pakistani population resides in the slum areas and 29% of the population lives below the poverty line, most of whom are daily wage earners4. In the absence of formal social security by the government, the poor in Pakistan fear hunger much more than the COVID-19; hence, meeting their basic needs is significant for enforcing the shutdown.
Pakistan government spent less than 1% of GDP on health budget; and hence, limited availability of enough appropriate equipment was another challenge. Pakistan had about 2000 ventilators and limited PPE equipment, which were insufficient to meet the demands of this outbreak. In order to meet the needs of frontline healthcare workers; orders were immediately placed for testing kits, personal protective equipment, ventilators, and other medical essential supplies, with local and international agencies. Additionally, a special compensation package was announced for the healthcare workers and hiring of additional healthcare force was initiated to meet the increasing demands. The government also set aside a budget for supporting scientists, researchers, and other experts to boost initiatives that could enhance the government’s capacity and capability in its fight against COVID-19.
The print and electronic media, non-governmental organisations (NGOs), and religious leaders also launched several initiatives. The media started playing a crucial role in creating awareness, providing updated information, promoting personal safety and social distancing norms, encouraging people to contribute in cash and kind, and in keeping the morale high of all frontline personnel, such as healthcare providers and law enforcement agents. The NGOs extended their support in various ways, for example, by identifying people who needed food and basic supplies and delivering these through experienced riders of commercial food chains. They also began providing support for disinfection spray activities in high-risk areas. Five-star hotels chipped in by distributing food parcels at hospitals to healthcare providers to acknowledge their services. The religious leaders contributed by spreading helpful information to prevent the spread of the disease and by reassuring the people via media and mosque announcements.
Additionally, the innovative contextual services such as tele-health, helpline, and tele-school television channel have been introduced. The government, in collaboration with the Aga Khan University Hospital, started the tele-consultation services on critical care issues, such as ventilator management for corona virus patients. In order to reduce the loss that the students were facing and to alleviate psychological effects associated with this pandemic, many schools, colleges, and universities have launched online teaching-learning programmes and the government has launched the tele-school television channel.
In the battle against coronavirus, the Pakistani scientists and researchers have also made remarkable intellectual contributions such as initiation of the authorized plasma therapy trials in early April 2020 and development of the passive immunization technique, using purified antibodies, which has been approved by the FDA, USA, for clinical trial5.
In Pakistan, the COVID-19 case fatality rate is much lower (1.7%) than in the developed countries (6.2%)6. The possible reasons for this difference could be the small fraction of 4% constitutes population aged 65 years and frequent daily hygienic practices during religious rituals. On the contrary, it might be the case of under-reporting which can be related to incidences where people have escaped from quarantine centres and hospitals. In addition, people in the lower socio-economic strata are not reporting if any family member or close one showed symptoms of the virus for fear of being isolated in the hospital and fear of their entire area/community being put under quarantine. The possible explanation of distress and panic among people could be the sub-optimal arrangements at quarantine facilities, insufficient resources at healthcare facilities, close-knitted family ties, and inability to attend funeral services of loved ones, separation anxiety, social boycott, and stigmatization. Nonetheless, Pakistan has its share of problems that are different from the developed world.
Future recommendations should aim to focus on the following:
1. Scientific research should concentrate more on devising digital rapid screening and testing procedures as well as vaccinations for limiting its spread.
2. Government should invest in sanitation facilities such as using WASH indicators.
3. The Surveillance system for COVID-19 should be streng-thened at the national and global levels.
4. More investment should be made to improve healthcare facilities and capacity building of all healthcare professionals.
5. The reach of telehealth facilities must be expanded to remote parts of the country whereby patients do not need to visit the traditional hospital setting for diagnosis and treatment.
6. The government must promote the initiatives to advance online teaching and learning practices which needs to be considered as a new direction for working from home and continuing education from home.
7. In order to promote high adherence to the prevention of this pandemic, the slogan and message of physical distancing from each other must be encourage
8. Self-isolation should be promoted for those who are able to manage at home, to minimise the stigma and cost.
9. Public-private partnership initiatives to encourage health insurance cover to general public that confront the issues of bearing the costs of treatment in such pandemics.
This pandemic has exhibited that predicament can strike at any time; thus it is imperative to start developing preventive and rapid response measures for such outbreaks in the future. Crucial interventions are needed to alleviate the potentially overwhelming effects of COVID19, by comprehending and minimising the long-term impact of this pandemic on frontline healthcare workers, quarantined people, and the general public. The spread of the pandemic is gradually increasing in Pakistan and the aforementioned recommendations will augment the efficiency of the current responses and initiatives. On a positive note, this pandemic can be a window of opportunity for governments of developing countries to reflect diligently while preparing national budget for healthcare system. Acknowledgment: Sumbul Khawaja, Trainee Nurse Intern, Aga Khan University Hospital Karachi Pakistan Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors
CONFLICT OF INTEREST:
Authors declared no conflict of interest.
AUTHORS’ CONTRIBUTION:
SF: Conception and design, drafting, final approval.
SIH: Conception, interpretation, critical revision, final approval.
SS: Design, critical revision, final approval.
YP: Interpretation, critical revision, final approval.
REFERENCES
- Van Bavel JJ, Boggio P, Capraro V, Cichocka A, Cikara M, Crockett M, et al. Using social and behavioural science to support COVID-19 pandemic response. Nat Hum Behav 2020; 4(5):460-71.
- WHO, Coronavirus disease 2019 (COVID-19) April 20, 2020 https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports.
- Government of Pakistan, April21, 2020, covid.gov.pk. COVID_19 Health Advisor Government of Pakistan.
- Asian Development Bank, Poverty Data: Pakistan Retrieved on April 21, 2020 https://www.adb.org/countries/pakistan/poverty.
- Pakistan doctors get approval for plasma therapy clinical, Gulf news, April 15, (2020):COVID-19: l trial https://gulf news.com/world/asia/pakistan/covid-19-pakistani-doctors-get-approval-for-plasma-therapy-clinical-trial-1.70988056from .
- Coronavirus cases fatality rate very low in Pakistan, Tribune, dated April 15, 2020 https://tribune.com.pk/story/2197999/1-covid-19-cases-fertility-rate-low-pakistan.