Embolisation of the Coronary Arterial Tree with Thick Contrast Material during Coronary Angiography
By Waleed M Ghaleb1, Abdelfatah Elasfar1, Mohsen Alarbash1, Abdulrahman Aldiri1, Abdulhalim Jamal Kinsara2Affiliations
doi: 10.29271/jcpsp.2021.04.466ABSTRACT
A 58-year male was referred to our centre with an acute inferior ST elevation myocardial infarction (STEMI). During the primary percutaneous coronary intervention, he suddenly collapsed with severe hypotension and severe bradycardia. The symptoms were attributed to an accidental embolisation of his left coronary system with the thick contrast material. When the remaining contrast in the bottle was investigated, it contained abnormally thick contrast material. This is a rare case of contrast embolisation, which is completely preventable but fatal, if undetected.
Key Words: Coronary angiography, Contrast material, Contrast embolisation.
INTRODUCTION
Coronary angiography is the gold standard test for identifying the presence and extent of atherosclerotic coronary artery disease (CAD) in patients presenting with acute coronary syndrome (ACS) as with any invasive procedure, specific patient-dependent and procedure-related complications are inherent to the test. Complications range widely from minor problems with short-term sequelae to life-threatening situations that may cause irreversible damage, if urgent care is not provided.1,2 The associated risks have decreased significantly with the inception of coronary arteriography due to advanced equipment design, improved peri-procedural management, and increased experience of diagnostic centres and operators.3 The most frequently documented side-effects of contrast media are benign, which rarely cause serious complications. We report a rare side-effect of contrast medium, which is the embolisation of the coronary tree with thick contrast material during coronary angiography.
CASE REPORT
A 58-year male, known to be a heavy smoker, was referred to our hospital with a history of typical angina for the last two hours. which was diagnosed as inferior ST elevation myocardial infarction (STEMI), as shown in his ECG (Figure 1).
He was given 600 mg of clopidogrel and 324 mg of acetylsalicylic acid and transferred directly to the catheterisation laboratory for primary percutaneous coronary intervention (PCI) as per local protocol.
After securing the arterial access, the patient was given a loading dose of heparin and tirofiban, according to the protocol. The left coronary system was cannulated first, using a 6 French left Judkins diagnostic catheter. After ensuring air removal from the catheter system, the left main coronary artery was engaged; and on injection of the contrast, the left anterior descending and left circumflex coronary arteries appeared hazy with a sluggish flow and multiple blockages due to multiple filling defects throughout the left coronary arterial system (Figures 2A and 2B). Initially, air bubbles were suspected, however, the shape of air embolism is clearly circumscribed, having a bubble shape, small in diameter with a clear cavity. The patient suddenly became hypotensive and bradycardiac. We promptly initiated resuscitative procedures including central femoral venous and arterial lines for possible use of an intra-aortic balloon pump. The patient received intravenous fluids, atropine, norepinephrine, and dopamine to support him hemodynamically. There was no arrhythmia on the monitor and no signs of electromechanical dissociation. He improved within minutes of initiating the resuscitation with normal vital signs (blood pressure, heart rate, oxygen saturation and mentation). The contrast injection system was checked and the contrast bottle was found to be cloudy with a thick contrast material (Figure 3). The shape of the coronary filling defect, due to the thick contrast embolisation, appeared irregular and moving slowly. It was a large diameter defect with no visible cavity in the middle, making air embolism unlikely to be the cause.
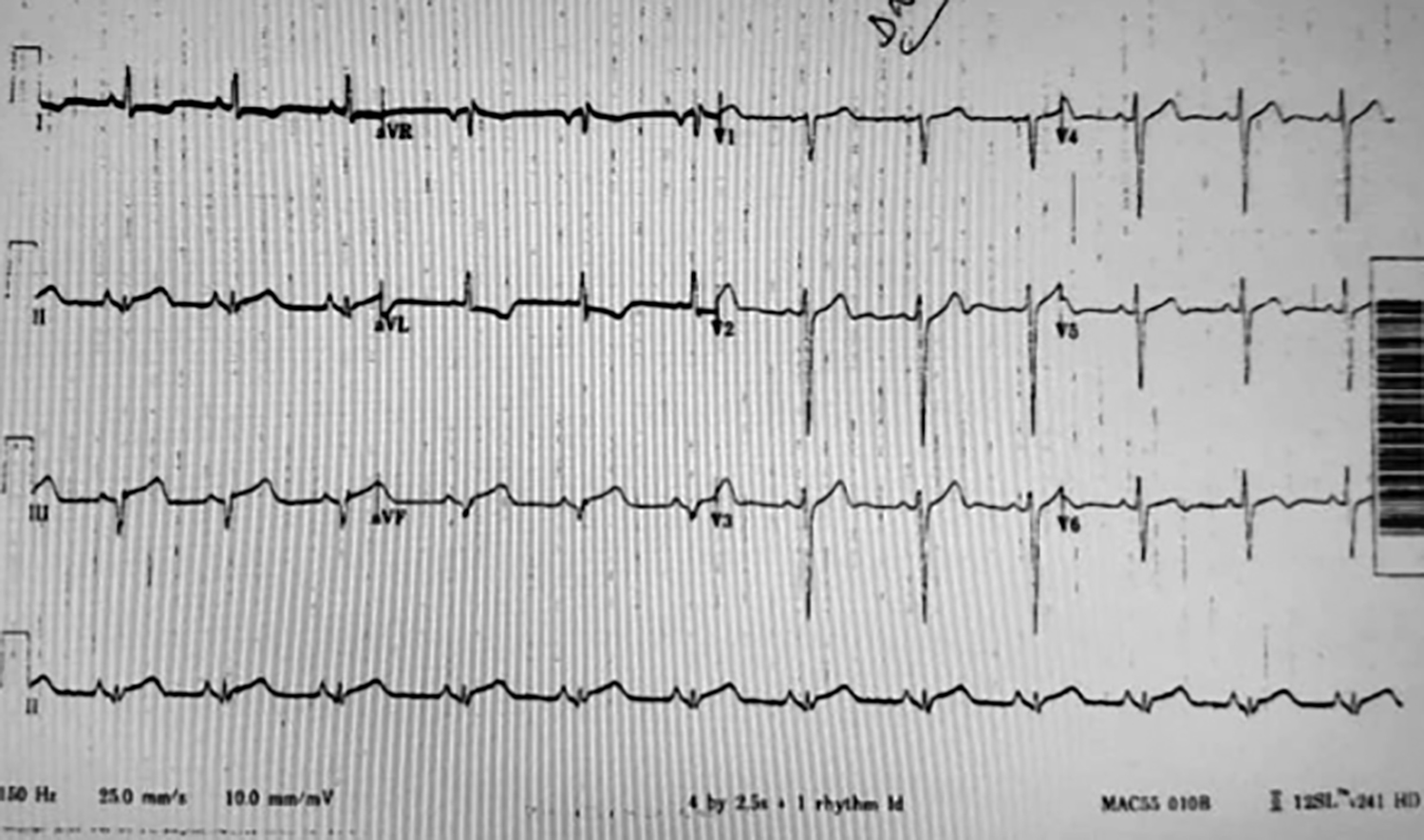 Figure 1: A 12-lead ECG tracing showing ST elevation in leads II, III and aVF.
Figure 1: A 12-lead ECG tracing showing ST elevation in leads II, III and aVF.
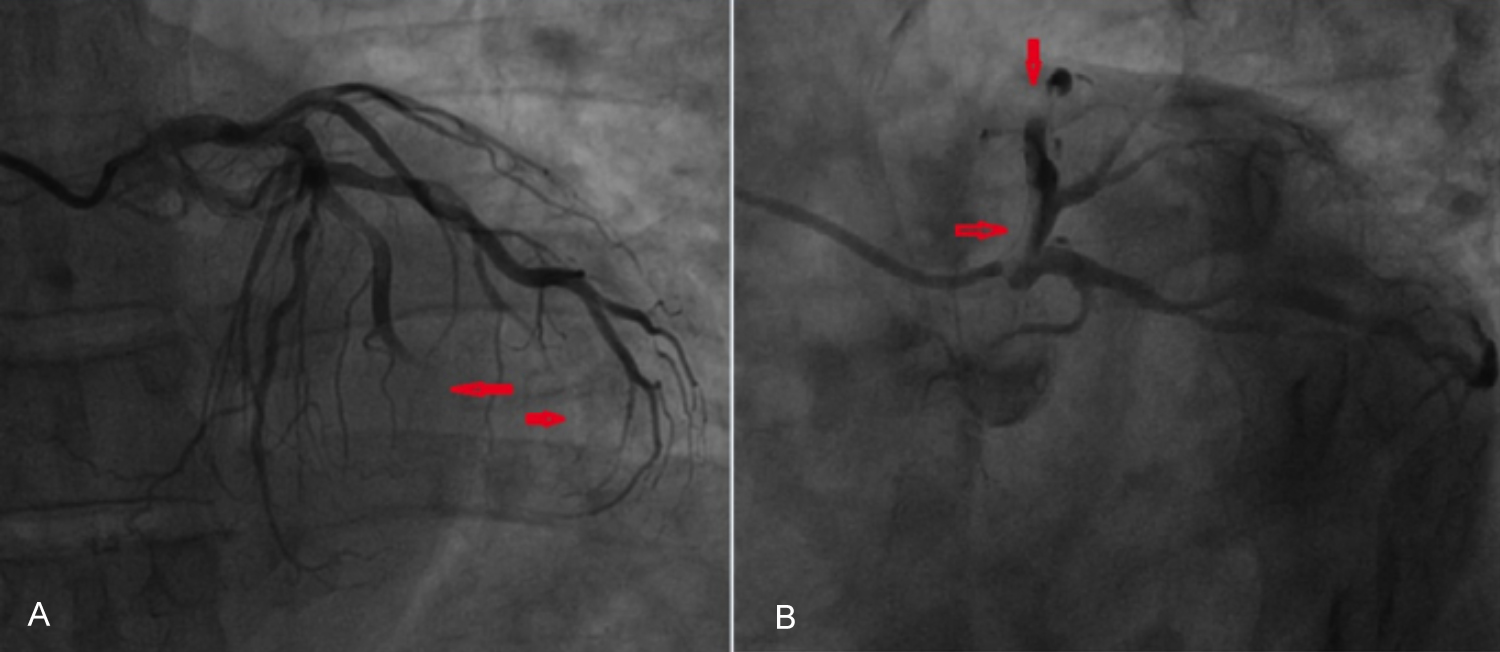 Figure 2: (A) Filling defects of left anterior descending left circumflex and obtuse marginal coronaries (arrows). (B) Thick contrast in the proximal left anterior descending artery (arrow).
Figure 2: (A) Filling defects of left anterior descending left circumflex and obtuse marginal coronaries (arrows). (B) Thick contrast in the proximal left anterior descending artery (arrow).
 Figure 3: The bad quality contrast, which was initially used on right of the image and the clear contrast bottle of the same type on the left of the image.
Figure 3: The bad quality contrast, which was initially used on right of the image and the clear contrast bottle of the same type on the left of the image.
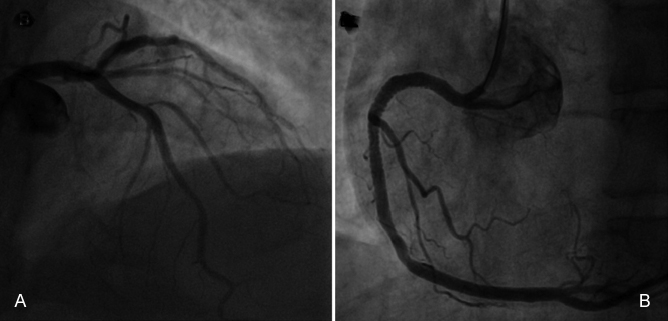 Figure 4: (A) Follow-up coronary angiogram after 24 hours of presentation showing clear left coronary system with TIMI III flow without any filling defect.(B) Final results after stent deployment to the right coronary artery (RCA) showing TIMI III flow.
Figure 4: (A) Follow-up coronary angiogram after 24 hours of presentation showing clear left coronary system with TIMI III flow without any filling defect.(B) Final results after stent deployment to the right coronary artery (RCA) showing TIMI III flow.
We routinely use an automated contrast injection machine, the ACIST device. The machine is prefilled with contrast by the radiographer technician and is far away from the coronary angio operator. Due to the use of an injector controller connected to the ACIST machine by a long wire, the color of the contrast was not noted by the operator. The expiry date was still valid. The procedure was resumed using another bottle with clear contrast and the right coronary artery (RCA) was injected using a 6F, Judkins right (JR) catheter, which revealed a proximal tight lesion of about 90% with a heavy thrombus burden.
The RCA lesion was managed by percutaneous transluminal coronary angiography (PTCA) (Figure 4), which resumed TIMI II flow distal to the lesion. After the angioplasty, the ST segment returned to the baseline. The patient was transferred to the coronary care unit (CCU) in a stable condition. A follow-up coronary angiogram was done after 24 hours, which revealed a completely normal left system and the RCA lesion was stented successfully (Figures 4A and 4B).
DISCUSSION
Adverse effects of contrast material can vary from an anaphylactic reaction to constitutional symptoms. Side-effects are self-limiting in the majority of cases. The most frequent contrast complications are allergy, nephropathy, thyroid abnormality; and in rare cases, acute pancreatitis.4-6 Coronary contrast embolisation is very rare and fatal, if not discovered and treated appropriately. To our knowledge and after searching the literature, no case of coronary contrast embolisation has been published; and this could be the first reported case. The cause of the abnormally thick contrast material is unknown, but may have been due to a brake in the storage chain from the main store to the customer or a manufacturer error. We store the contrast medium in a specially designed space at a temperature of 5°C-25°C and the catheterisation laboratory is cooled to the recommended temperature. The incident was reported to the manufacture and we did not find other bottle with the same abnormal consistency in the same store. The change in the contrast medium may be related to a temperature change. In dogs, preheating contrast medium to body temperature was shown to reduce the risk of serious cardiovascular complications.7 Old types of contrast media caused platelet degranulation. The change in contrast color may reflect a change in the physical properties of the contrast used in this cae.8 Our patient was managed successfully with supportive measures.
The aim of reporting this case is to share with other practitioners the small unpredictable errors that can be fatal in emergency situations, especially during primary urgent procedures. All equipment should be checked prior to any procedure to avoid such fatal avoidable errors.
In conclusion, we report the first case of contrast embolisation, which can be prevented easily; but can prove fatal, if undetected.
PATIENT'S CONSENT:
Written informed consent was obtained from the patient for his anonymised information to be published in this article.
CONFLICT OF INTEREST:
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
AUTHORS' CONTRIBUTION:
All contributed equally to the preparation and the revision of the manuscript. All authors read and approved the final manuscript.
REFERENCES
- Andreucci M, Solomon R, Tasanarong A. Side-effects of radiographic contrast media: Pathogenesis, risk factors, and prevention. BioMed Res Int 2014; 2014:741018. doi: 10.1155/2014/741018.
- Sutton A, Finn P, Grech E. Early and late reactions after the use of iopamidol 340, ioxaglate 320, and iodixanol 320 in cardiac catheterisation. Am Heart J 2001; 141(4):677-83. doi: 10.1067/mhj.2001.113570.
- Tavakol M, Ashraf S, Brener SJ. Risks and complications of coronary angiography. Glob J Health Sci. 2012; 4(1):65-93. doi: 10.5539/gjhs.v4n1p65.
- Davenport MS, Khalatbari S, Dillman JR, Cohan RH, Caoili EM, Ellis JH. Contrast material-induced nephrotoxicity and intravenous low-osmolality iodinated contrast material. Radiology 2013; 267(1):94-105. doi: 10.1148/radiol. 12121394.
- Bonelli N, Rossetto R, Castagno D, Anselmino M, Vignolo F, Parasiliti Caprino M, et al. Hyperthyroidism in patients with ischaemic heart disease after iodine load induced by coronary angiography. Clin Endocrinol (Oxf) 2018; 88(2): 272-8. doi: 10.1111/cen.13494.
- Gorges R, Ghalayini W, Zughaib M. A case of contrastinduced pancreatitis following cardiac catheterisation. J Invasive Cardiol 2013; 25(10):E203-4.
- Jacobsen EA, Mortensen E, Refsum H, Kløw NE. The effect of the temperature of contrast media on cardiac electrophysiology and hemodynamics during coronary arteriography. Invest Radiol 1992; 27(11):942-6.
- Chronos NA, Goodall AH, Wilson DJ, Sigwart U, Buller NP. Profound platelet degranulation is an important side effect of some types of contrast media used in interventional cardiology. Circulation 1993; 88 (5 Pt 1):2035-44. doi: 10.1161/01.cir.88.5.2035.