Complete Prolapse of a Giant Upper Rectal Adenoma
By Feng Chi, Shenkang ZhouAffiliations
doi: 10.29271/jcpsp.2021.03.363
Sir,
Rectal adenomas are common polyps of significant concern, which are closely related to rectal cancers and considered precancerous lesions.1 With the introduction of colorectal cancer screening, the number of adenomas detected has increased.2 Early rectal adenoma removal can reduce rectal cancer incidence.3 Therefore, all confirmed rectal adenomas should be surgically removed.
The management of large rectal adenomas or those in the upper rectum is tricky.4 Transanal surgery and endoscopic surgery are the most commonly used techniques to treat rectal adenomas. These approaches enable local adenoma removal; and have advantages over other techniques, such as transsacral resection, transabdominal approach, and transanal total mesorectal excision; in that, they are less invasive, have faster recovery times, and confer a lower risk of complications. The transanal surgical approach for rectal adenomas is the simplest and most economical, but it is generally applicable for adenomas in the lower or mid rectum. Because of the large distance from the anus and poor surgical vision, transanal resection of adenomas in the upper rectum is difficult. Endoscopic surgery is another important technique for resecting rectal adenomas, suitable for adenomas in the upper rectum. However, large rectal adenomas are difficult to remove endoscopically. Moreover, it is more time-consuming and expensive than traditional transanal excision. Since both the transanal and endoscopic approaches have positive and negative aspects, we believe a combination of these approaches could be a better procedure.
A 49-year man presented to the Emergency Department of Taizhou Hospital of Zhejiang Province with complaints of a mass protruding per anus, abdominal pain, and bleeding for one hour. He had a history of overt haematochezia for three months, but none of a protruding mass per anus previously. Physical examination showed a soft abdomen without tenderness. Rectal examination revealed a giant, fleshy, frond-like mass (about 5 × 4 cm) protruding from the anal verge (Figure 1). The mass could not be reduced by gentle pressure.
The patient underwent emergent surgery. Initially, transanal local resection of the mass was planned. However, owing to lack of the operator’s experience, the mass retracted back into the rectum during manual anal dilation. Subsequently, the retracted mass was neither palpable by digital rectal examination, nor visible anoscopically. Colonoscopy confirmed the mass in the upper rectum (10 cm from the anal verge) (Figure 2). Under colonoscopy, a laparoscopic grasping forceps was used to clamp the tumour pedicle. Subsequently, the mass was pulled close to the anus, and transanal local resection was performed. The recovery was uneventful. Histological examination revealed a tubular adenoma with negative margins as the final diagnosis.
A giant upper rectal adenoma can be treated by a combination of the colonoscopic and transanal approaches. This procedure should be recommended as a possible option in the treatment of lesions in the upper rectum.
 Figure 1: Photograph of mass protruding per anus.
Figure 1: Photograph of mass protruding per anus.
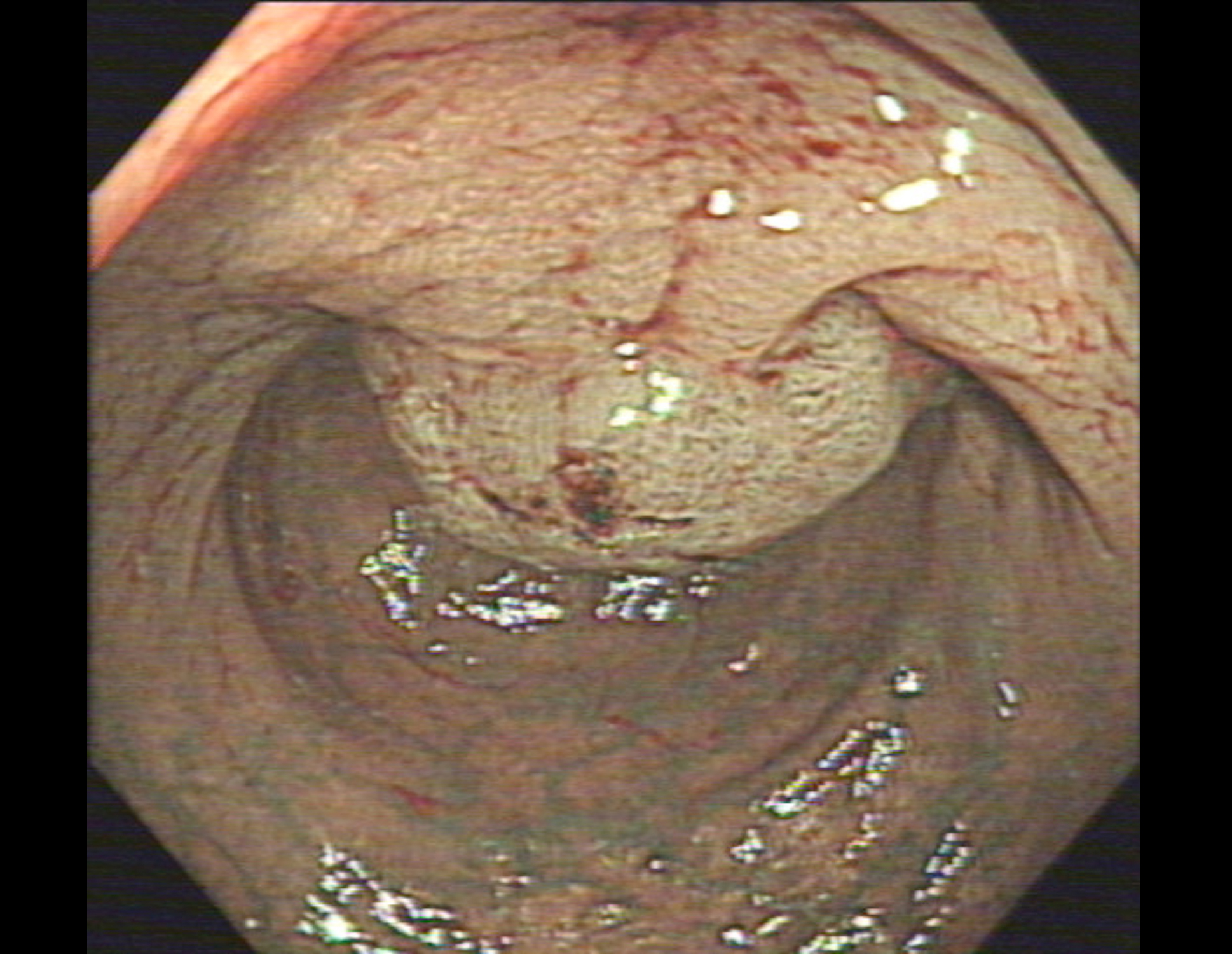 Figure 2: A colonoscopic examination revealed a giant pedunculated tumour in the rectum, located 10 cm proximal to the anal verge.
Figure 2: A colonoscopic examination revealed a giant pedunculated tumour in the rectum, located 10 cm proximal to the anal verge.
PATIENT’S CONSENT:
Informed verbal and written consent was taken both for the surgery and pictures, and details of the case to be included.
CONFLICT OF INTEREST:
The authors declared no conflict of interest.
AUTHORS’ CONTRIBUTION:
FC: Surgery, paper writing and literature review.
SZ: Literature review, and manuscript revision.
REFERENCES
- Winawer SJ, Zauber AG, Ho MN, O’Brien MJ, Gottlieb LS, Sternberg SS, et al. Prevention of colorectal cancer by colonoscopic polypectomy. The national polyp study workgroup. N Engl J Med 1993; 329:1977-81.
- Van Rijn AF, Dekker E, Kleibeuker JH. Screening the population for colorectal cancer: The background to a number of pilot studies in the Netherlands. Ned Tijdschr Geneeskd 2006; 150:2739-44.
- Zauber AG, Winawer SJ, O’Brien MJ, Lansdorp-Vogelaar I, van Ballegooijen M, Hankey BF, et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med 2012; 366:687-96.
- Arezzo A, Arolfo S, Cravero F, Migliore M, Allaix ME, Morino M. Which treatment for large rectal adenoma? Preoperative assessment and therapeutic strategy. Minim Invasive Ther Allied Technical 2014; 23:21-7.