Association of Gonial Angle on Panoramic Radiograph with the Facial Divergence on Lateral Cephalogram
By Saad Abdul Rehman1, Sadia Rizwan2, Syed Shah Faisal1, Syed Sheeraz Hussain1Affiliations
doi: 10.29271/jcpsp.2020.04.355ABSTRACT
Objective: To find the mean gonial angle values among different facial divergent cases.
Study Design: Cross-sectional descriptive study.
Place and Duration of Study: Karachi Medical and Dental College from October 2018 to December 2019.
Methodology: Panoramic radiographs (OPG) and lateral cephalograms of 91 patients, 33 males and 58 females, were obtained. Sella-Nasion-Mandibular Plane (SNMP) angle was measured on lateral cephalogram and gonial angles were measured on panoramic radiograph. Subjects were divided into three groups as per SNMP angle as hypodivergent, normodivergent and hyperdivergent. A p-value of less than 0.05 was considered statistically significant.
Results: The mean value of the gonial angle in OPG among all the patients was 125.05° with a standard deviation 7.24°. The average gonial angle in males was 124.10° ±5.67° and in females was 125.59° ±7.99°. Out of 91 patients, 14 were hypodivergent, 28 were normodivergent and 49 were hyperdivergent. The mean values of gonial angle among these three groups were 119.77° ±6.05°, 123.66° ±5.50° and 127.36° ±7.52°. One-way ANOVA demonstrated highly significant differences in the values of gonial angles among three facial divergences (p=0.001). Post-Hoc Tukey analysis showed that there was a significant difference between gonial angle of hyperdivergent and hypodivergent cases (p=0.001).
Conclusion: Gonial angle on panoramic radiographs (OPG) may provide useful knowledge about the facial divergence of the orthodontic patients.
Key Words: Gonial angle, Facial divergence, Lateral cephalogram, Panoramic radiograph, Orthodontic diagnosis.
INTRODUCTION
Cephalogram and orthopantomogram (OPG) radiographs are routinely taken for every orthodontic patient for diagnostic purpose.1 Paatero introduced the panoramic radiography which provides important information about the bony skeleton of head and neck, the teeth, their positions, their inclinations, period of maturation, and the tissues surrounding it.2
Cephalometric analysis helps to evaluate the vertical and horizontal relationships of the various bones making up face, cranium, cranial base and dentition. The vertical, horizontal and transverse relationships of these structures are important for treatment planning, and the outcome which is affected by the vertical relationships and the growth pattern of the patient.3
Sella-Nasion-Mandibular Plane (SNMP) angle is a very important angular measurement which is formed by the intersection of two horizontal lines SN (Sella-Nasion) and MP (Mandibular plane).4-6
There are three basic types of vertical facial patterns; namely, long face (hyperdivergent, high angle case), average face (normodivergent, normal angle case) and short face (hypodivergent, low angle case).7
The gonial angle is significant for the diagnosis of craniofacial skeletal disorders. This parameter may give an indication about the vertical parameters and symmetry of the facial skeleton. It can be measured on both radiographs (OPG and lateral Cephalogram).8,9 Larheim et al. suggested that lateral cephalograms do not provide gonial angle’s accurate and fully reliable registration because the bilateral structures in craniofacial complex superimpose and create hurdles in identification, registration and measurement of the gonial angle, whereas its assessment on OPG X-rays was nearly identical to the angle measured on the dried mandible.10
There is a huge gap exist in the literature of orthodontics regarding examining the panoramic radiograph as a tool of investigation of vertical skeletal patterns. It can be used for reliable measurement of the gonial angle as there is no complication of images of superimposed structures appearing as in cephalograms.11
Previously, authors worked on association and correlation of gonial angles on panoramic radiograph and lateral cephalogram.12 However, no study has been done which worked on the association of gonial angle on panoramic radiograph and vertical skeletal patterns on lateral cephalogram.
The purpose of the present study was to find out the mean values of gonial angle among the three facial groups on panoramic radiograph.
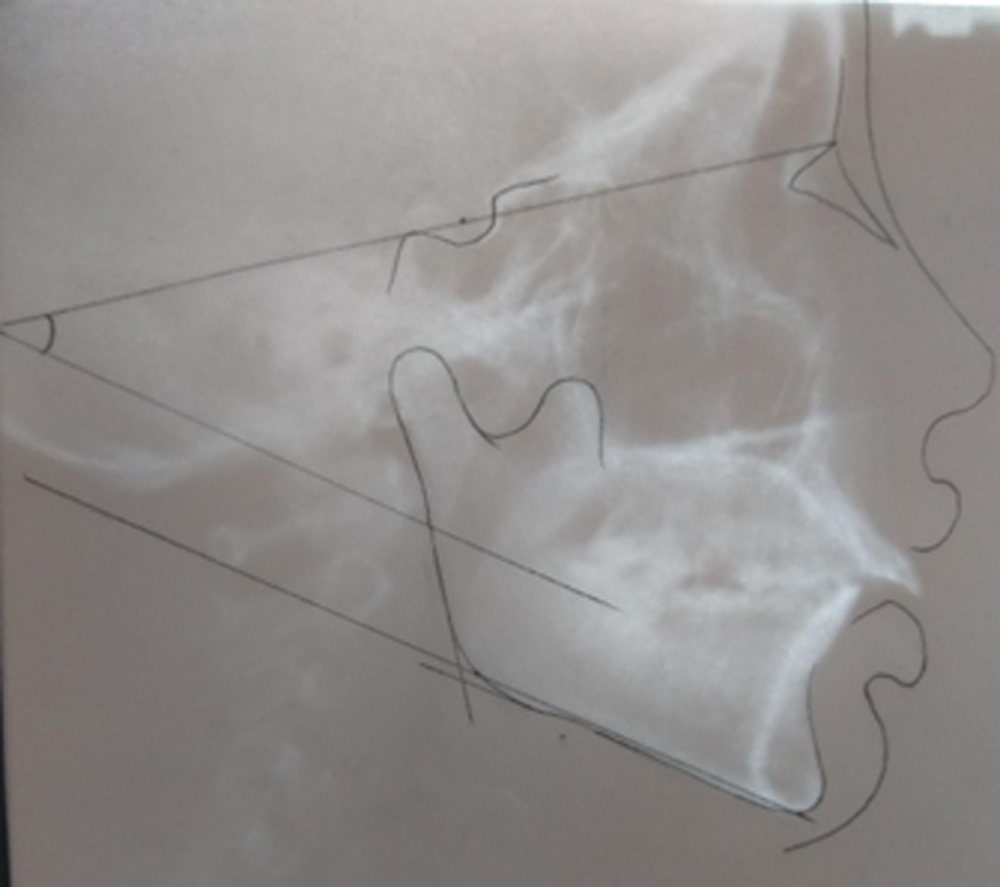 Figure I: SNMP angle measurement on lateral cephalogram.
Figure I: SNMP angle measurement on lateral cephalogram.
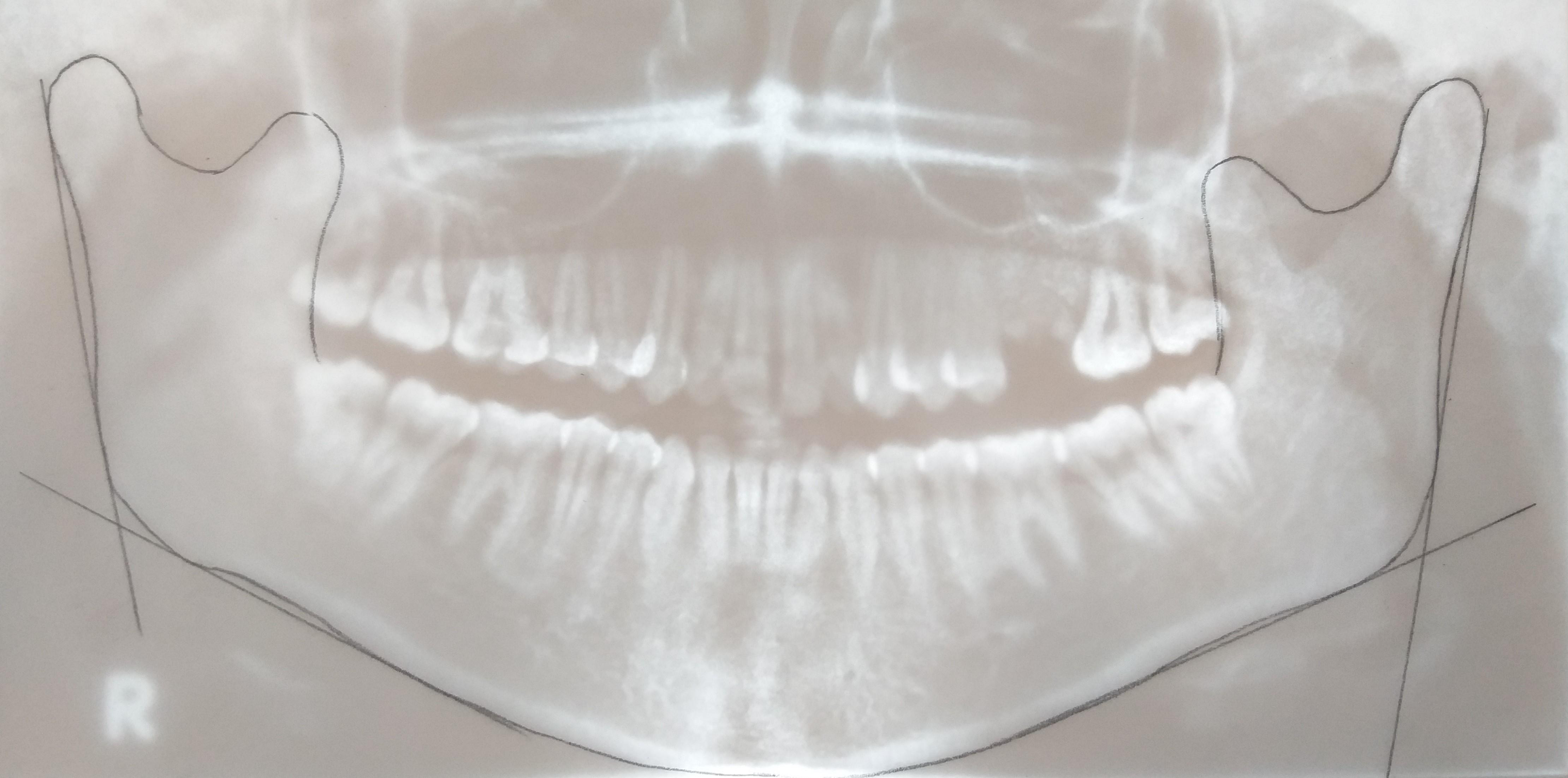 Figure 2: Gonial angle measurement on OPG.
Figure 2: Gonial angle measurement on OPG.
METHODOLOGY
The study was approved by the Ethical and Scientific Review Committee of Karachi Medical and Dental College. Non-probability consecutive method was used for sampling. Panoramic radiographs (OPG) and lateral cephalograms of 91 patients, were obtained from the patients visited to the Department of Orthodontics. Inclusion criteria were subjects of both gender seeking orthodontic treatment and exhibiting clear visibility of all required parameters on radiographs (Gonial angle and SNMP angle). Exclusion criteria were individuals having any known systemic disease, Cleft lip and/or palate, history of any facial trauma or surgical procedure of jaws and previous orthodontic treatment. All the patients were physically examined. SNMP angle was measured on lateral cephalogram (Figure 1) and gonial angles were measured on panoramic radiograph (Figure 2). Subjects were divided into three groups as per SNMP angle as hyperdivergent: more than 36 degree, hypodivergent: less than 28 degree and normodivergent: between 28 to 36 degree.
To measure the gonial angle, a line was drawn on the panoramic radiographs (traced on cellulose sheet or butter paper with 0.5mm pointed pencil) tangential to the lower border of the mandibular body; another line was drawn tangential to the posterior borders of the ramus and the condyle. The intersection of these two lines formed the gonial angle as shown in Figure 2.13 It was measured on both sides and average was taken.
The data was analysed statistically using software IBM SPSS statistics version 20. The statistical analysis involved calculation of mean and standard deviation of gonial angle and frequencies along with percentages of qualitative variables like gender and groups of facial divergences. One-Way ANOVA test was used to fulfill our aim of study, followed by Post-Hoc Tukey analysis.
Table I : Mean values of gonial angle among three different groups.
|
Facial divergence |
Mean and std. deviation |
N (%) |
F-value |
p-value |
|
Hypodivergent |
119.77 ±6.05 |
14 (15.4) |
7.742 |
0.001 |
|
Normodivergent |
123.66 ±5.50 |
28 (30.8) |
||
|
Hyperdivergent |
127.36 ±7.52 |
49 (53.8) |
||
|
Total |
125.05 ±7.24 |
91 (100.0) |
Table II : Difference between groups.
|
Facial divergence |
p-value |
95% confidence interval |
|
|
Hypodivergent |
Normodivergent |
0.188 |
-9.16 – 1.37 |
|
Hyperdivergent |
0.001 |
-12.47 – -2.71 |
|
|
Normodivergent |
Hypodivergent |
0.188 |
-1.37 – 9.16 |
|
Hyperdivergent |
0.059 |
-7.51 – 0.12 |
|
|
Hyperdivergent |
Hypodivergent |
0.001 |
2.71 – 12.47 |
|
Normodivergent |
0.059 |
-0.12 – 7.51 |
|
|
*The mean difference is significant at the 0.05 level. |
|||
RESULTS
There were 91 patients including 36.26% (N=33) males with the mean age of 17.2 ±4.4 years and 63.74% (N=58) females with the mean age of17.03 ±4 years. The mean value of the average gonial angle in OPG among all the patients was 125.05° with a standard deviation 7.24°. The average gonial angle in male was 124.10°±5.67° and in female was 125.59° ±7.99°. Out of 91 patients, 14 were hypodivergent, 28 were normodivergent and 49 were hyperdivergent. The mean values of gonial angle among these three groups were 119.77° ±6.05°, 123.66° ±5.50° and 127.36° ±7.52° (Table I). One-way ANOVA demonstrated highly significant differences in the values of gonial angles among three facial divergences with the p-value of 0.001. Post-Hoc Tukey analysis showed that there is a significant difference between gonial angle of hyperdivergent and hypodivergent cases with the p-value of 0.001 (Table II).
DISCUSSION
The gonial angle describes the form and the shape of the mandible which plays a vital role in predicting and forecasting the growth pattern of an individual. The goal of this study was an effort to enhance the panoramic radiograph’s clinical use by determining its potential use for evaluating skeletal vertical pattern. Very few studies have been published, which involves the use of panoramic radiographs in evaluating gonial angle measurements.
Usually, cephalometric measurements and analysis are used to investigate craniofacial growth and its pattern. This study extends the current use of panoramic radiograph by exploring the link between gonial angle identified on panoramic radiograph and SNMP angle on lateral cephalogram.
This study was conducted to reduce the unnecessary X-ray exposure while determining the vertical skeletal pattern and it could be a step towards the diagnosis of orthodontic patients with a single radiograph. The average expected dose from a lateral cephalogram is 3 µSv, which indicates a very little risk with the chances of malignancy being less than 1 patient per million and reduction in the amount of possible exposure from lateral cephalogram would be beneficial for patients.14,15
Alhaija et al. evaluated and explained the potential of panoramic radiographs to measure mandibular inclination which directly effects skeletal vertical pattern. They concluded that panoramic radiograph is a useful tool for the measurement of gonial angle, which clearly indicates the mandibular inclination and steepness. Alhija’s remarks supported our study in indirect way that panoramic radiograph can be used to determine mandibular steepness or skeletal vertical pattern. They compared and correlated gonial angles on both radiographs unlike our research in which we found association of gonial angle on OPG and facial divergence on lateral cephalogram. Thus, the ability to determine the growth direction from a panoramic radiograph is useful because most dentists advice a panoramic radiograph for patients during routine dental examinations.16 Shahabi et al. also conducted study with using same parameters and found the results same as Alhaija et al. found.17
Akcam et al. also tried to establish a link between skeletal patterns determined in lateral cephalogram with the panoramic radiograph and remarked, “Though panoramic radiographs provide information on the vertical dimensions of craniofacial structures; however, clinicians should be careful when predicting skeletal cephalometric parameters from panoramic radiographs, because of their lower predictability percentages.”18
Svanaes concluded that linear measurements were unreliable. Therefore, it has been suggested that only angular measurements were used on the panoramic radiographs for studying skeletal pattern. The gonial angle reflects the form of the mandible and its value can be used to predict mandibular direction of growth. It also effects and influences the lip seal and competence and facial profile along with the angulation of the mandibular incisors. Its evaluation also provides the important information about stability of treatment.19
This study will definitely enable orthodontists to spot skeletal vertical pattern using a single radiograph, thereby avoiding the excessive exposure of radiations to the patients. It is recommended that further studies should include larger sample size and use of other variables for the diagnosis of vertical skeletal pattern addition to the SNMP angle.
CONCLUSION
A panoramic radiograph (OPG) can provide knowledge about the facial divergence of the patient through the gonial angles measurement, which can be a useful tool for categorizing skeletal vertical pattern.
ETHICAL APPROVAL:
Ethical and Scientific Review Committee of Karachi Medical and Dental College (Reference No. 016/18).
PATIENTS’ CONSENT:
Written informed consents were obtained from patients who participated in this study.
CONFLICT OF INTEREST:
All authors declared no conflict of interest.
AUTHORS’ CONTRIBUTION:
SAR: Contributed substantially to the conception and design of the study, the acquisition of data, or the analysis and interpretation.
SR: Provided critical revision of the article.
SSF: Helped and supervised the project and also provided critical revision of the article.
SSH: Helped in the conception and design of the study. He also gave final approval of the version to publish.
All authors discussed the results and contributed to the final manuscript.
REFERENCES
- Manosudprasit A, Haghi A, Allareddy V, Masoud MI. Diagnosis and treatment planning of orthodontic patients with 3-dimensional dentofacial records. Am J Orthod Dentofacial Orthop 2017; 151:1083-91.
- Kundi I. Accuracy of assessment of gonial angle by both hemispheres of panoramic images and its comparison with lateral cephalometric radiographic measurements. J Dent Health Oral Disord Ther 2016; 4:00116.
- Livas C, Delli K, Spijkervet FK, Vissink A, Dijkstra PU. Concurrent validity and reliability of cephalometric analysis using smartphone apps and computer software. Angle Orthod 2019; 89:889-96.
- Gonzalez MB, Caruso JM, Sugiyama RM, Schlenker WL. Establishing cephalometric norms for a Mexican population using Ricketts, Steiner, Tweed and Arnett analyses. APOS Trends in Orthodontics 2013; 3:171-7.
- Ahmed M, Shaikh A, Fida M. Reliability of various skeletal indicators in assessing vertical facial soft tissue pattern. J Ayub Med Coll Abbottabad 2016; 28:7-13.
- Bawane SS, Andrade NN. Hard and soft tissue changes following maxillary distraction osteogenesis and mandibular setback with bilateral sagittal split osteotomy. J Maxillofac Oral Surg 2016; 15:491-500.
- Sampson P, Little RM, Årtun J, Shapiro PA. Long-term changes in arch form after orthodontic treatment and retention. Am J Orthod Dentofacial Orthop 1995; 107:518-30.
- Delaire J, Schendel SA, Tulasne JF. An architectural and structural craniofacial analysis: A new lateral cephalometric analysis. Oral Surg Oral Med Oral Pathol 1981; 52:226-38.
- El-Bialy T, Aboul-Azm SF, El-Sakhawy M. Study of craniofacial morphology and skeletal maturation in juvenile diabetics (Type I). Am J Orthod Dentofacial Orthop 2000; 118:189-95.
- Belaldavar C, Acharya AB, Angadi P. Sex estimation in Indians by digital analysis of the gonial angle on lateral cephalo-graphs. J Forensic Odontostomatol 2019; 37:45-50.
- Bhullar MK, Uppal AS, Kochhar GK, Chachra S, Kochhar AS. Comparison of gonial angle determination from cephalograms and orthopantomogram. Indian J Dent 2014; 5:123-6.
- Zangouei-Booshehri M, Aghili HA, Abasi M, Ezoddini-Ardakani F. Agreement between panoramic and lateral cephalometric radiographs for measuring the gonial angle. Iran J Radiol 2012; 9:178-82.
- Lone EA, Mushtaq M. Comparison of gonial angle on lateral cephalogram and orthopantomogram in class i class ii and class iii cases-a cross sectional study. Annals of International Medical and Dental Research 2018; 4:35.
- Khan WA, Faisal SS, Hussain SS. Correlation of craniofacial measurements between cephalometric radiographs and facial photographs. Annals Abbasi Shaheed Hospital & Karachi Medical & Dental College 2018; 23:37-45.
- Giuca MR, Pasini M, Drago S, Del Corso L, Vanni A, Carli E, et al. Influence of vertical facial growth pattern on Herbst appliance effects in prepubertal patients: A retrospective controlled study. Int J Dent 2020; 2020.
- Alfawzan AA. Gonial angle as a determinant of gender, a panoramic study in a sample of saudi population. Indian J Public Health Res & Dev 2020; 11:1732-6.
- Shahabi M, Ramazanzadeh BA, Mokhber N. Comparison between the external gonial angle in panoramic radiographs and lateral cephalograms of adult patients with Class I malocclusion. J Oral Sci 2009; 51:425-9.
- Akcam MO, Altiok T, Ozdiler E. Panoramic radiographs: A tool for investigating skeletal pattern. Am J Orthod Dentofacial Orthop 2003; 123:175-81.
- Ganeiber T, Bugaighis I. Assessment of the validity of orthopantomographs in the evaluation of mandibular steepness in Libya. J Orthod Sci 2018; 7:14.