Fishbone-induced Pericardial Hemorrhage Resulting in a Misdiagnosis of Acute Myocardial Infarction
By Zuoan Qin, Liagnqing GeAffiliations
doi: 10.29271/jcpsp.2022.04.9ABSTRACT
Fishbone intake is a common clinical event; but serious complications resulting from the ingestion of fishbones, such as perforations in the stomach, diaphragm, and pericardium and heart lacerations, are rare. Here, we present a case of fishbone-induced pericardial hemorrhage that led to a misdiagnosis of acute myocardial infarction (AMI) since the emergency coronary angiogram showed normal coronaries. However, the patient’s circulatory status was not good and an echocardiogram revealed pericardial effusion. A contrast-enhanced computed tomography (CT) of the chest and abdomen showed a foreign body in the upper abdomen. Therefore, an urgent exploratory thoracotomy was performed, and it was discovered that the pericardial hemorrhage was caused by the fishbone puncturing the pericardium and myocardium of the right ventricle. The fishbone was removed, damaged vessels were repaired, and the pericardium was closed with a drain. The patient was discharged in good clinical condition. In order to avoid unnecessary damage and suffering, the possibility of a foreign body in the esophagus or heart must be considered when patients have chest pain, and careful reporting of histories and corresponding examinations are necessary.
Key Words: Acute myocardial infarction, Fishbone, Pericardial effusion.
INTRODUCTION
Acute chest pain is a common clinical symptom. Common causes include acute coronary syndrome, aortic dissection, and acute abdomen; however, they are also rarely the symptoms caused by foreign bodies in the upper gastrointestinal tract.1 We present a case of a fishbone penetrating the pericardium and causing cardiac injury that was misdiagnosed as acute myocardial infarction (AMI).
CASE REPORT
A 55-year male presented with central chest pain that gradually moved to the right side of the face. There was no previous medical history of heart problems. On physical examination, he was hypotensive with blood pressure (BP) of 100/70 mmHg with tachypnea. His electrocardiogram (ECG) showed ST elevation in leads I, II, III, and V4 – V6 (Figure 1), with raised troponin I level (0.34 ng/ml). A diagnosis of AMI was made, but his coronary angiogram showed no coronary artery disease. Chest CT revealed pericardial effusion and a pericardial puncture extracted 70 ml of blood, confirming the diagnosis of hemopericardium (Table I).
Table I: Timeline of events.
|
Date |
Time |
Event |
|
Day 1 |
17:30 |
Acute thoraco-abdominal pain. |
|
Day 2 |
10:00-11:30 |
Local hospital (Emergency percutaneous coronary angiography and Pericardial puncture). |
|
Day 3 |
00:30 |
Emergency Department of our hospital. |
|
|
00:30-02:00 |
Thoracic Surgery. |
|
|
02:11 |
Transfer to the intensive care unit. |
|
|
03:30 |
Pericardial drainage. |
|
|
06:00 |
Enhanced thoraco-abdominal CT. |
|
|
10:00 |
General hospital consultation. |
|
|
11:38-13:08 |
Emergency thoracotomy and pericardial exploration. |
|
|
15:00 |
Transferred to the thoracic surgery general ward. |
|
Day 6 |
08:17 |
Extubation. |
|
Day 8 |
|
Switch to thoracic surgery general ward. |
|
Day 11 |
|
Discharged. |
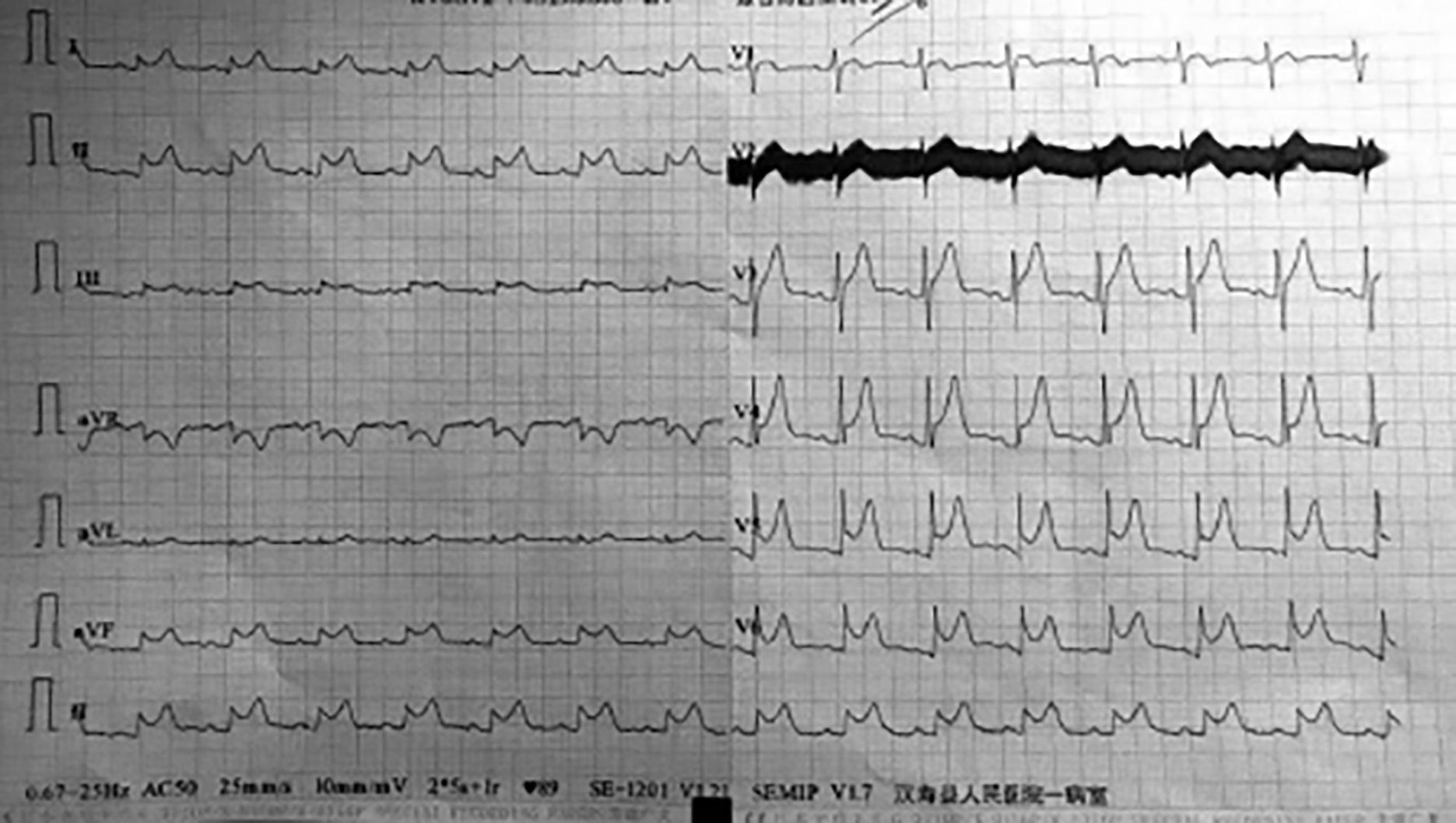 Figure 1: First electrocardiography (ECG).
Figure 1: First electrocardiography (ECG).
 Figure 2: Chest and abdomen linear CT. (A) Coronal section; (B) Sagittal section; (C) Transverse section.
Figure 2: Chest and abdomen linear CT. (A) Coronal section; (B) Sagittal section; (C) Transverse section.
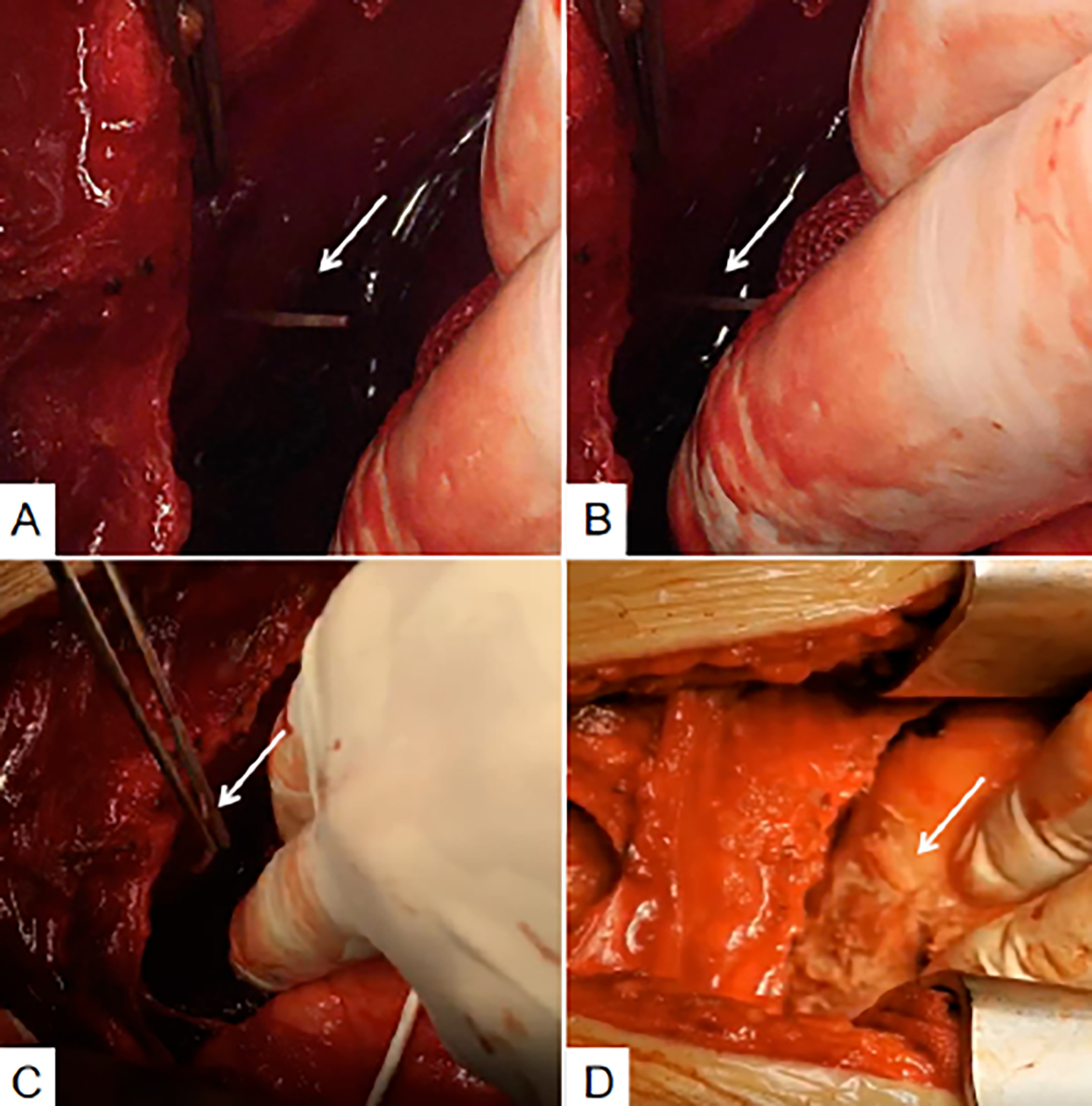 Figure 3: (A and B) Fishbone puncturing through diaphragm and pericardium. (C) Extracting the fishbone. (D) Medical glue with pericardial slice to close heart wound.
Figure 3: (A and B) Fishbone puncturing through diaphragm and pericardium. (C) Extracting the fishbone. (D) Medical glue with pericardial slice to close heart wound.
 Figure 4: Extracted fishbone.
Figure 4: Extracted fishbone.
Due to respiratory failure and persistent hypotension, he was ventilated and transferred to the intensive care unit (ICU). Dopamine was administered for muscle support. The cardiologist performed a two-dimensional echo examination that showed cardiac tamponade due to excessive hemopericardium, and a second pericardial puncture drew 200 ml of blood. The liquid drawn from the nasogastric tube showed blood-stained extracts. Contrast-enhanced CT of the chest and abdomen showed foreign bodies in the lower chest, suggesting that those foreign bodies came from the esophagus and/or stomach; and caused pericardial perforation and heart damage (Figure 2). The patient underwent endotracheal general anesthesia; and emergency thoracotomy and pericardium exploratory surgery was performed (Figure 3). We found a fishbone, approximately 3.5 cm in length (Figure 4) that had penetrated the stomach, diaphragm, pericardium, and myocardium of the right ventricle. The surgeon closed the heart and pericardium wounds with medical glue. The general surgeon observed that the abdominal septum had been adhered, and the abdominal cavity was clean. The operation was performed without any complications.
DISCUSSION
Inadvertent ingestion of fishbone is a common situation; however, only approximately 1% will cause gastrointestinal perforation, which is a rare clinical condition.2,3 The existing literature shows that acute pericardial effusion due to esophageal or heart damage caused by swallowed fishbone is uncommon.4-7 Pericardial hemorrhage caused by accidental swallowing of a fishbone is very rare in clinical practice; and because patient history is often not adequately obtained, it is likely to be misdiagnosed as AMI, as in our case. His emergency coronary angiography was negative, but the local hospital chest CT examination showed pericardial effusion. After the pericardial puncture, the patient's pericardial hemorrhage continued. The cause of the bleeding was unclear, which eventually caused the symptoms of cardiac tamponade. The patient was in shock before being transferred to a tertiary care hospital. After another pericardial puncture and drainage, the patient's condition improved temporarily; but the pericardial bleeding and fluid containing blood removed from the gastric tube drainage were highly suggestive of a foreign body injury. Contrast-enhanced CT of the abdomen and chest revealed a foreign body that had penetrated the stomach and pericardium. After the family’s consent, an exploratory thoracotomy was performed. A final diagnosis of pericardial hemorrhage induced by fishbone puncturing the gastric wall, diaphragm, and pericardium, and scratching the coronary blood vessels of the heart was made.
When reviewing the entire treatment process, there are many aspects worthy of reflection. The clinician responsible for the first consultation failed to check and sufficiently question the patient about his medical history. The main clinician at the local hospital did not read the chest CT in person, which led to misdiagnosis. At the same time, the patient's ECG showed typical changes of acute pericarditis that account for 5% of presentations with acute chest pain; however, the patient was misdiagnosed.5-7 Chest CT is the technique of choice when foreign bodies are suspected to be in the digestive tract.8,9 In this case, the fishbone was completely inside the mediastinum. CT, because of its high-density resolution, can reveal smaller fishbone and complications such as bleeding and abscesses of the esophagus and its surrounding tissues, so it has important guiding significance for clinical diagnosis. However, the smaller fishbones are prone to be missed. Therefore, when no foreign body is found in conventional CT scans of patients with mediastinal foreign body, thin-layer CT scans should be taken. Finally, the negative result of the emergency coronary angiography, leads to the failure to re-examine the chest and abdomen CT scans in time, and resulted in further deterioration of the patient's condition. Situations like these can be life-threatening if left untreated. Clinicians should rule out other common causes as soon as possible. At the same time, they should also consider such rare causes and actively perform relevant examinations to confirm a diagnosis.
In conclusion, for patients with thoraco-abdominal pain, it is necessary to consider the possibility that foreign bodies in the digestive tract could be the cause. Careful history-taking and appropriate examinations can help avoid unnecessary damage and protect patients from needless pain.
PATIENT’S CONSENT:
Written consent was taken from the patient.
CONFLICT OF INTEREST:
The authors declared no conflict of interest.
AUTHORS’ CONTRIBUTION:
ZQ: Writing – original draft, data collection and follow-up.
LG: Literature search and final draft of the case report.
REFERENCES
- Goodacre S, Cross E, Arnold J, Angelini K, Capewell S, Nicholl J. The health care burden of acute chest pain. Heart 2005; 91(2):229-30. doi: 10.1136/hrt.2003.027599.
- Webb WA. Management of foreign bodies of the upper gastrointestinal tract: Update. Gastrointest Endosc 1995; 41(1):39-51. doi: 10.1016/s0016-5107(95)70274-1.
- Goh BK, Chow PK, Quah HM, Ong HS, Eu KW, Ooi LL, et al. Perforation of the gastrointestinal tract secondary to ingestion of foreign bodies. World J Surg 2006; 30(3): 372-7. doi: 10.1007/s00268-005-0490-2.
- Ismail TF. Acute pericarditis: Update on diagnosis and management. Clin Med 2020; 20(1):48-51. doi: 10.1007/ s00268-005-0490-2.
- Sharland MG, McCaughan BC. Perforation of the esophagus by a fishbone leading to cardiac tamponade. Ann Thorac Surg 1993; 56(4):969-71. doi: 10.1016/0003-4975(93) 90368-r.
- Wang QQ, Hu Y, Zhu LF, Zhu WJ, Shen P. Fishbone-induced myocardial injury leading to a misdiagnosis of AMI: A case report. World J Clin Cases 2019; 7(20):3335-40. doi: 10. 12998/wjcc.v7.i20.3335.
- Hokama A, Uechi K, Takeshima E, Kobashigawa C, Iraha A, Kinjo T, et al. A fishbone perforation of the esophagus. Endoscopy 2014; 46 Suppl 1:216-7. doi: 10.1055/s-0034- 1364952.
- Birk M, Bauerfeind P, Deprez PH, Häfner M, Hartmann D, Hassan C, et al. Removal of foreign bodies in the upper gastrointestinal tract in adults: European society of gastrointestinal endoscopy (ESGE) clinical guideline. Endoscopy 2016; 48(5):489-96. doi: 10.1055/s-0042- 100456.
- Goh BK, Tan YM, Lin SE, Chow PK, Cheah FK, Ooi LL, et al. CT in the preoperative diagnosis of fishbone perforation of the gastrointestinal tract. AJR Am J Roentgenol 2006; 187(3):710-4. doi: 10.2214/AJR.05.0178.