Duodenal Ulcer Perforatıon after Actıvated Charcoal Treatment
By Nazmi Ozer, Abdullah SahinAffiliations
doi: 10.29271/jcpsp.2022.08.S107ABSTRACT
Activated charcoal, having the capacity to absorb substances with its porous surface, has been used in intoxication treatment for nearly 200 years. Although live-saving, occasionally, it can lead to complications. Because of the risk of perforation during activated charcoal therapy, the integrity of the gastrointestinal tract should be checked after the procedure.
In this case report, a 27-year patient, who received activated charcoal therapy after diclofenac intoxication developed duodenal ulcer perforation and charcoal peritonitis. The present case constitutes the first report of duodenal ulcer perforation after activated charcoal therapy.
It should be remembered that activated charcoal, which is widely used in intoxication treatment, may cause gastrointestinal system perforation, peritonitis, adhesion, abscess formation, organ loss within the abdomen, and prolonged hospitalization.
Key Words: Activated charcoal, Intoxication, Duodenal ulcer perforation.
INTRODUCTION
Activated charcoal is a carbon product exposed to heat and oxidized to increase its surface area. The porous surface of coal has the capacity to absorb substances. The use of activated charcoal in the cases of intoxication has been going on for nearly two centuries.
Activated charcoal acts both by absorbing a wide variety of toxins in the gastrointestinal tract and by increasing the elimination of toxins if systemic absorption has occurred. Oral activated charcoal can be given in a single dose or multiple doses. The absorptive capacity of charcoal depends on the natural properties of the local environment, such as the nature of the toxin and pH.1
Because of the nasogastric tube used during the administration of activated charcoal or during gastric lavage and due to the risk of perforation, the integrity of the gastrointestinal tract must be checked after the procedure.
In this case report, we present a case of charcoal peritonitis due to duodenal ulcer perforation occurring after the administration of activated charcoal, which to our best knowledge, represents the first case reported in the literature.
CASE REPORT
A 27-year male prisoner, who did not have any disease history and no previous surgery in his patient history and family history, visited the doctor for myalgia that started about 1 week ago. Diclofenac sodium (50 mg) tablet was prescribed by the prison doctor. The patient used the drug once a day for 1 week, then took 15 diclofenac sodium tablets (750 mg) for suicide, and was brought to the emergency service. On arrival at the emergency, his vital signs were stable, and his hemogram and biochemical tests were normal. There was no complaint of abdominal pain. Gastric lavage and activated charcoal were administered to the patient. The patient was followed up in the emergency room because of diclofenac's side effects such as intestinal irritation, bleeding, and hepatic and renal toxicity. He was discharged after 8 hours after physical examination, controlled hemogram, and biochemical examinations without any pathology.
About 24 hours later, the patient was brought back to the emergency room with the complaint of severe abdominal pain and there were signs of generalised peritonitis on the abdominal examination. Widespread sensitivity and rebound tenderness were positive in all quadrants. Laboratory investigations showed white blood cell ( WBC) count of 15,000/µL, hemoglobin of 16.3 g/dl, platelet count of 273,000/µL, and c-reactive protein (CRP), 168 mg/L. Biochemical tests were normal. Upon demonstration of free air under the diaphragm on radiography of the abdomen in standing posture, he was taken to the operation room with the pre-diagnosis of gastrointestinal system perforation.
Laparotomy was performed. During the exploration, minimal liquid substance, black-colored and sticky material covering the omentum, was observed in the abdomen. In addition, a perforation was found on the anterior wall of the duodenal bulb, approximately 0.5 cm in diameter (Figures 1 and 2). On reviewing the patient's history, it was observed that activated charcoal was administered 1 day before due to intoxication. It was clear that black matter was activated charcoal. Although the abdomen was washed with plenty of isotonic salines, some of the activated charcoal could not be removed from the tissues. Perforation was repaired with the Graham technique and 2 Jackson pratt drains were placed in the abdomen; one adjacent to the perforation area and the second in the rectovesical area. During the operation, a nasogastric tube was inserted for gastric decompression and drainage.
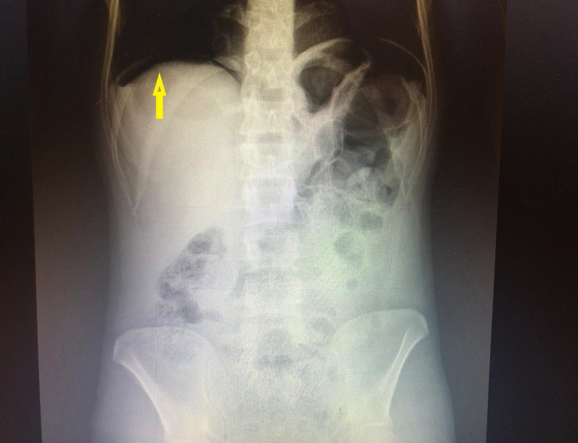 Figure 1: Abdominal X-ray in standing position. Free air can be seen under the diaphragm (yellow arrow).
Figure 1: Abdominal X-ray in standing position. Free air can be seen under the diaphragm (yellow arrow).
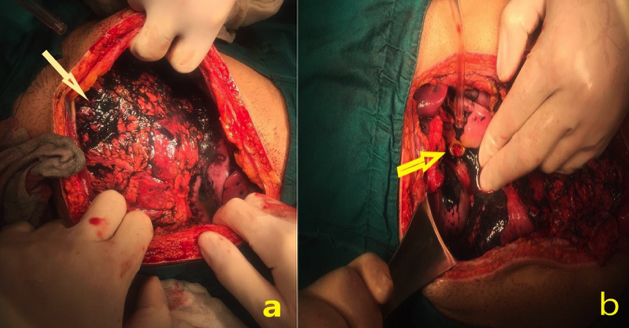 Figure 2: (a) Activated charcoal deposits (arrow) in the omentum inside the abdomen. (b) Duodenal ulcer perforation area (arrow) among the coal deposits.
Figure 2: (a) Activated charcoal deposits (arrow) in the omentum inside the abdomen. (b) Duodenal ulcer perforation area (arrow) among the coal deposits.
Antibiotic therapy (piperacillin and tazobactam, 4+4.5 g) was started and he was taken to the intensive care unit for post-operative care. Nexium (Proton pump inhibitor) treatment was given 40 mg/day. He was hydrated daily with 3000 cc fluid (1500 cc isotonic saline + 1500 cc 5% dextrose). Washing water used for abdominal cleansing during the surgery came out from abdominal drains measuring about 100 cc and black in color in the post-operative period. In the follow-up, the contents of the patient's lower abdominal drain turned purulent on 6th day. Culture from drain fluid was positive for Klebsiella pneumonia. The patient's antibiotic was changed to meropenem 3×1 g/day and moxifloxacin 1×400 mg/day. Wound discharge started from the incision. In the follow-up, the wound site of the patient developed midline evisceration. Under general anaesthesia, the patients peritoneal cavity was washed with an ample amount of isotonic saline. Abdominal skin was re-sutured with retention sutures and vacuum wound closure (VAC) treatment was started. After 20 days of VAC treatment, the patient's wound discharge regressed. WBC and CRP values returned to normal.
There was no fluid discharge from the abdominal drains, and the drains were removed. He was discharged on the 30th postoperative day.
DISCUSSION
Activated charcoal is a carbon product used as a therapeutic agent in many cases of intoxication.2,3 In addition to gastrointestinal decontamination, it stops the enterohepatic and enterovascular cycle and prevents toxin conversion.4 In studies on volunteers, a single dose of activated charcoal has been shown to absorb poison and reduce gastrointestinal absorption.5 Some activated charcoal applications are performed with gastric lavage. Esophageal perforation and activated charcoal mediastinitis may develop during application.6,7 Also in one patient with a history of Roux-n-Y gastric bypass operation, after the gastric lavage and activated charcoal application, perforation occurred and the patient developed coal peritonitis, which was initially suspected to be a case of endometriosis.8 Our case is the first in the literature with the development of duodenal ulcer perforation and activated charcoal peritonitis following the application of activated charcoal. Diclofenac intoxication with the absence of a known history of duodenal ulcer made us suspect whether the perforation is due to gastrointestinal irritation of diclofenac sodium or a mechanical event due to nasogastric irritation, or an active coal-related perforation. However, regardless of the cause of perforation, as seen in our case, activated charcoal appears to be a serious irritant in the abdomen and can lead to infectious complications.9 Because of this irritant feature, we think it may cause duodenal ulcer perforation or it may help perforation by increasing duodenal irritation due to diclofenac sodium poisoning.
During the treatment of intoxication, it should be remembered that the commonly used activated charcoal can be a cause of perforation of the gastrointestinal tract, recurrent peritonitis, adhesions, abscess formation, and solid organ loss in the abdomen, leading to the prolonged hospital stay.
FINANCIAL DISCLOSURE:
The authors declared that this study has received no financial support
PATIENT’S CONSENT:
Informed consent was obtained from the patient who participated in this study.
COMPETING INTEREST:
The authors declared no competing interest.
AUTHORS’ CONTRIBUTION:
NO: Concept, supervision, data collection and / or processing, writing manuscript, critical reviews.
AS: Design, analysis and /or interpretation, literature search.
All authors approved the final version of the manuscript to be published.
REFERENCES
- Park GD, Spector R, Goldberg MJ. Johnson GF, Feldman R, Quee CK. Effect of the surface area of activated charcoal on theophylline clearance. J Clin Pharmacol 1984; 24(7): 289-92. doi: 10.1002/j.1552-4604.1984.tb01835.x.
- Proudfoot AT. Abandon gastric lavage in the accident and emergency department? Arch Emerg Med 1984; 1(2): 65-71. doi: 10.1136/emj.1.2.65.
- Vale JA, Proudfoot AT. How useful is activated charcoal? BMJ 1993; 306(6870):78-9. doi: 10.1136/bmj.306.6870.78.
- Levy G. Gastrointestinal clearance of drugs with activated charcoal. N Engl J Med 1982; 307(11):676-8. doi: 10. 1056/NEJM198209093071109.
- Maurer HH. Demands on scientific studies in clinical toxicology. Forensic Sci Int 2007; 165(2-3).2-3:194-8. doi: 10.1016/j.forsciint.2006.05.019.
- Lanphear WF. Gastric lavage. J Emerg Med 1986; 4(1): 43-7. doi: 10.1016/0736-4679(86)90111-3.
- Caravati EM, Knight HH, Linscott MS Jr, Stringham JC. Esophageal laceration and charcoal mediastinum complicating gastric lavage. J Emerg Med 2001; 20(3): 273-6. doi: 10.1016/s0736-4679(01)00282-7.
- Dunning K, Plymyer MR. Charcoal peritonitis causing chronic pelvic pain: A unique complication following bariatric surgery. Obes Surg 2006; 16(9):1238-42. doi: 10.1381/096089206778392121.
- Mariani PJ, Pook N. Gastrointestinal tract perforation with charcoal peritoneum complicating orogastric intubation and lavage. Ann Emerg Med 1993; 22(3):606-9. doi: 10. 1016/s0196-0644(05)81954-7.