Acrometastasis of Laryngeal Carcinoma to the Finger
By Cengiz Karacin1, Sema Turker1, Dogan Yazilitas1, Tulay Eren1, Tugba Taskin Turkmenoglu2Affiliations
doi: 10.29271/jcpsp.2022.04.55ABSTRACT
Distant metastasis of laryngeal carcinoma occurs at the rate of 4%-12%, with the most common sites being the lungs, liver and bone. Acrometastasis occurs rarely in cases of laryngeal carcinoma; to date, only three cases of acrometastasis have been reported. Herein, we describe a 66-year male, who was followed up for metastatic laryngeal carcinoma and developed paronychia. Hot compress was applied, antibiotic treatment was administered, and fine-needle biopsy of the lesion was performed. The lesion did not regress despite the administration of a broad-spectrum antibiotic. The results of cytological examinations were consistent with squamous cell carcinoma metastasis.
Rarely occurring acrometastases indicate poor prognosis in cancer patients; expected survival is short and treatment is usually palliative. In such cases, finger amputation or local radiotherapy are recommended. Clinicians should be aware when treating metastatic laryngeal cancer that such atypical lesions as paronychia can be associated with the primary tumour.
Key Words: Acrometastasis, Laryngeal carcinoma, Finger, Metastasis.
INTRODUCTION
Worldwide, laryngeal carcinoma occurs in >100,000 individuals annually.1 Distant metastasis of laryngeal carcinoma occurs at the rate of 4%-12%, with the most common sites being the lungs, liver and bone.2 To date, only three cases of acrometastasis in laryngeal carcinoma patients have been reported.3-5 Acrometastasis occurs rarely in other types of cancer, as well. A review of 70 cases of acrometastasis reported that lung cancer patients accounted for 32.9%, renal cell carcinoma (RCC) patients for 20%, breast cancer patients for 12.9%, and colon cancer patients accounted for 10%.6
Paronychia develops due to inflammation of the lateral and proximal nail folds. It is usually observed in individuals, who habitually bite their fingernails or suck their fingers and in patients with diabetes mellitus.7 In mild cases of acute paronychia, treatment with a hot compress is usually sufficient. In cases with a more aggressive course, antibiotic treatment is administered and the abscess, if present, is drained.8
Herein, we describe a rare case of clinically diagnosed paronychia, who did not respond to proper treatment and was subsequently determined to be metastatic laryngeal carcinoma. To the best of our knowledge, the presented case is only the fourth to be described.
CASE REPORT
A 66-year male presented with hoarseness of voice and underwent laryngoscopic examination, which showed the presence of a mass. The biopsy of the mass confirmed the diagnosis of laryngeal squamous cell carcinoma (SCC). The disease was locally advanced (T3N2bM0) at the time of diagnosis. Although not routinely practised, a combination of docetaxel + cisplatin + 5 fluorouracil (DCF) chemotherapy was administered, followed by chemoradiotherapy in an attempt to downsize the tumour. Complete response to the treatment was observed upon follow-up clinical and radiological evaluation; however, recurrence occurred 11 months post-treatment — a soft-tissue lesion was observed at the base of the skull. Unilateral neck dissection was performed and the mass was excised from the base of the skull. The findings of histopathological analysis of the mass excision were compatible with SCC and the patient underwent stereotactic radiosurgery at another institution. As the patient did not return for follow-up, concomitant therapy was not administered at the time. Thoracic CT performed 16 months after recurrence showed bilateral metastatic nodules in the lung. Then cisplatin + 5 fluorouracil + cetuximab was initiated as the first-line treatment.
After the first cycle of first-line treatment, swelling with pain developed in the patient’s left-hand fourth finger (Figure 1). SCC metastasis and paronychia were considered in the differential diagnosis. Hot compress was applied, antibiotic treatment was administered, and fine-needle biopsy of the lesion was performed. The lesion did not regress despite administration of broad-spectrum antibiotic therapy. PET/CT was performed, based on the suspicion of bone and other distant organ metastases, which showed metastatic lesions in the lungs, cervical lymph nodes, and distal phalanx of the left-hand fourth finger. The results of cytological examinations were consistent with SCC metastasis (Figure 2). The patient was advised amputation for acrometastasis, followed by nivolumab therapy, but he declined all treatments. It was later learned that the patient had died 6 weeks later from the discharge.
 Figure 1: Swollen left-hand fourth finger.
Figure 1: Swollen left-hand fourth finger.
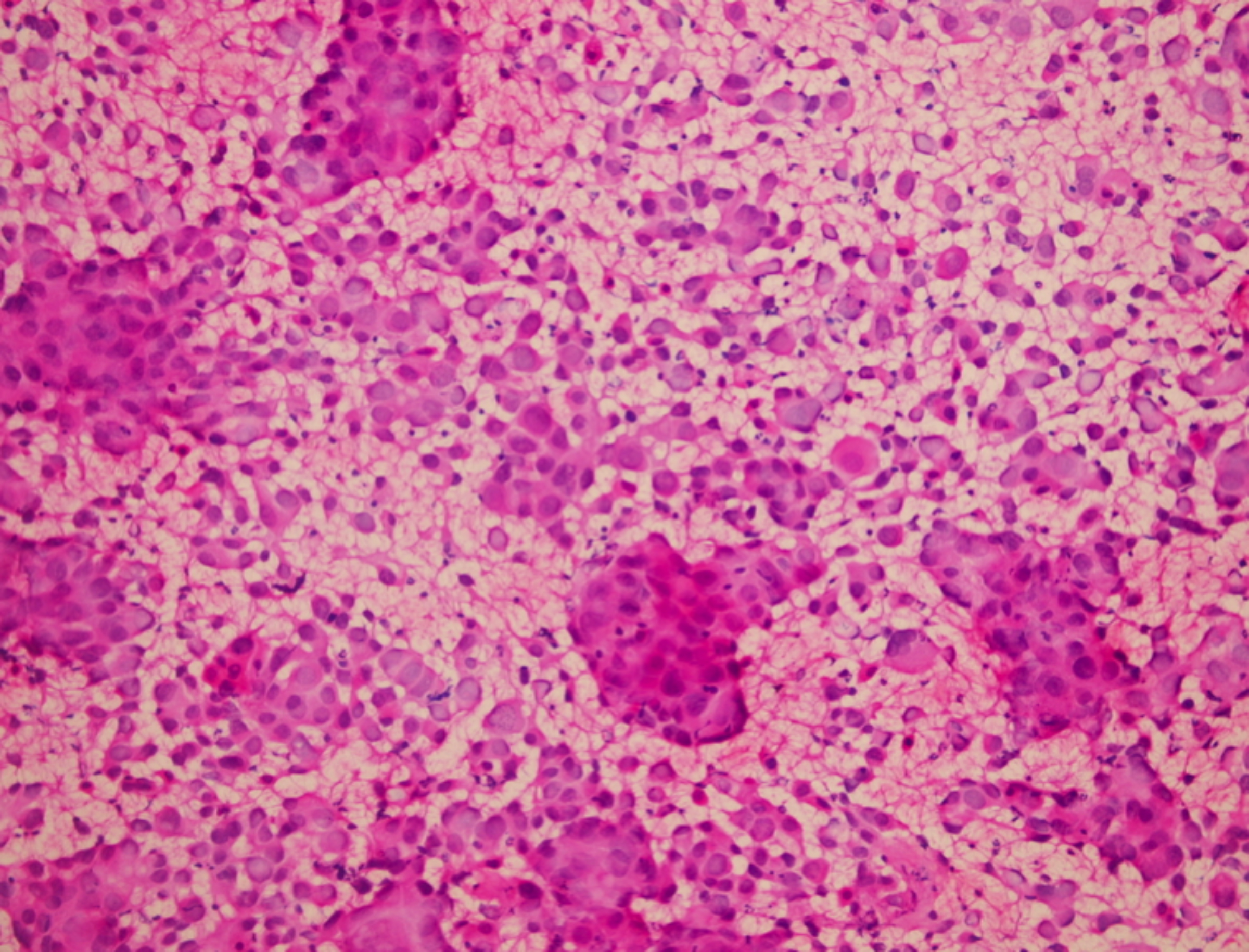 Figure 2: Cytological features of the tumour cells.
Figure 2: Cytological features of the tumour cells.
DISCUSSION
In cases of laryngeal cancer, distant metastasis commonly occurs in the lungs, bones and liver; whereas, it rarely occurs in skin.2 To date, there have only been three reported cases of acrometastases in laryngeal carcinoma patients.3-5 Diagnosis is made, based on cytological and histopathological confirmation of the lesion.4 In the presented case, diagnosis was confirmed histopathologically.
One report describes a case of laryngeal carcinoma with lung and finger metastases.4 It was suggested that the tumour cells might have undergone acrometastasis via direct implantation from pulmonary secretions; as the patient, who underwent total laryngectomy, had used his thumb to perform tracheoesophageal speech. In contrast, in another case acrometastasis occurred in ≥ 2 fingers, suggesting that acrometastasis can develop in lung cases as well.6 The fact that lung metastasis occurs in most acrometastasis cases also suggests hematogenous spread as the mechanism of metastasis, rather than direct implantation of tumour cells.6
We think that such metastases might develop via capillary embolisms, associated with circulating tumour cells. Acrometastasis occurs very rarely, but affects survival negatively. When acrometastasis does occur, expected survival is short and treatment is usually palliative.9 Kumar et al.5 reported that their patient with metastatic laryngeal carcinoma died two months after the diagnosis of acrometastasis. The present patient died six weeks after the diagnosis of acrometastasis, supporting the notion that acrometastasis is a poor prognostic factor in cases of laryngeal carcinoma.
In addition to controlling systemic disease, local treatments aimed at eliminating symptoms associated with acrometastasis should also be considered. Such local treatments can help improve patients’ quality of life. As such, finger amputation or local radiotherapy are recommended in cases of solitary acral metastasis.10 Clinicians should be aware when treating metastatic laryngeal cancer that such atypical lesions as paronychia can be associated with the primary tumour.
PATIENT’S CONSENT:
The patient provided written informed consent to publish his case prior to his death.
CONFLICT OF INTEREST:
The authors declared no conflict of interest.
AUTHORS’ CONTRIBUTIONS:
CK: Manuscript writing.
ST: Manuscript writing and patient recruitment.
DY: Proofreading.
TE: Data collection.
TTT: Figures and data collection.
REFERENCES
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin 2014; 64(1):9-29. doi: 10.3322/caac.21208.
- Spector, JG, Sessions DG, Haughey BH, Chao KS, Simpson J, El Mofty S, et al. Delayed regional metastases, distant metastases, and second primary malignancies in squamous cell carcinomas of the larynx and hypopharynx. Laryngoscope 2001; 111(6):1079-87. doi: 10.1097/0000 5537-200106000-00028.
- Nayak J, Zhong Y, Haigentz M Jr. Acral metastases from laryngeal carcinoma. J Clin Oncol 2011; 29(9): 220-1. doi: 10.1200/JCO.2010.32.3543.
- Lewin JS, Cleary KR, Eicher SA. An unusual metastasis to the thumb in a laryngectomized tracheoesophageal speaker. Arch Otolaryngol Head Neck Surg 1997; 123(9): 1007-9. doi: 10.1001/archotol.1997.01900090123020.
- Kumar N, Bera A, Kumar R, Goshal S, Angurana SL, Srinivasan R. Squamous cell carcinoma of supraglottic larynx with metastasis to all five distal phalanges of left hand. Indian J Dermatol 2011; 56(5):578-80. doi: 10.4103/ 0019-5154.87161.
- Stomeo D, Tulli A, Ziranu A, Perisano C, De Santis V, Maccauro G. Acrometastasis: A literature review. Eur Rev Med Pharmacol Sci 2015; 19(15):2906-15.
- Shroff PS, Parikh DA, Fernandez RJ, Wagle UD, Clinical and mycological spectrum of cutaneous candidiasis in Bombay. J Postgrad Med 1990; 36(2):83-6.
- Wollina, U. Acute paronychia: Comparative treatment with topical antibiotic alone or in combination with corticosteroid. J Eur Acad Dermatol Venereol 2001; 15(1): 82-4.
- Afshar A, Farhadnia P, Khalkhali H. Metastases to the hand and wrist: An analysis of 221 cases. J Hand Surg Am 2014; 39(5):923-32.e17. doi: 10.1016/j.jhsa.2014.01.016.
- Cole RD, McGuirt WF. Prognostic significance of skin involvement from mucosal tumors of the head and neck. Arch Otolaryngol Head Neck Surg 1995; 121(11):1246-8. doi: 10.1001/archotol.1995.01890110024004.