Contributions and Challenges of Radiology in the Era of COVID‐19 Pandemic
By Mahnoor Hafeez, Amjad SattarAffiliations
doi: 10.29271/jcpsp.2020.06.84Sir,
COVID‐19 is caused by a highly contagious RNA virus, belonging to the category of coronaviruses. It has created a disastrous impact on the world population. The fields of imaging and microbiology are playing key roles in diagnostics. Radiology has come forward in the battle zone because of few reasons: first of all, there is a limitation of RT PCR corona test that its sensitivity varies from 42-71%; and then there are false negatives -29%. Scarcity of test kits is another issue with prolong result turnaround time up to 24 hrs.
Chest radiograph and plain chest CT are the workhorse of imaging for lung parenchymal assessment in COVID pneumonia (Figures 1). There is a specific radiographic scoring system, in which a score of 0-4 has been assigned as [0- no involvement, 1:25%, 2:25-50%, 3:50-75%, 4: >75%] on the extent of lung parenchymal involvement. However, the chest film may be insensitive early in disease as compared to CT.
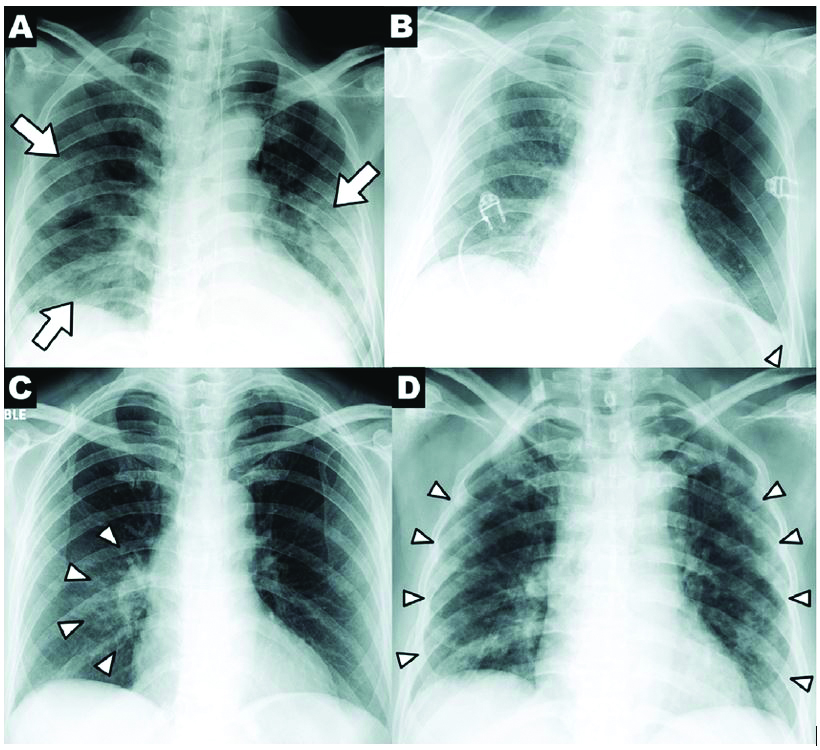 Figure 1: Chest X-ray findings in COVID-19: Patchy consolidations and GGO bilaterally (arrows).
Figure 1: Chest X-ray findings in COVID-19: Patchy consolidations and GGO bilaterally (arrows).
CT scan leads from radiography, because it has 100% specificity in COVID pneumonia.
Shi H et al. documented that abnormal findings were observed on CT chest in 100% of the 81 confirmed cases of COVID‐19 infection at Wuhan; this suggests CT scans also needs to be done in asymptomatic high risk patients.1 Salehi et al. reviewed 30 studies in 919 patients to conclude that the CT patterns in COVID-19 were ground glass opacification (GGO) - 88.0%, bilateral involvement - 87.5%, peripheral sub-pleural distribution-76%, and multi-lobe involvement in 78.8% of patients.2 Other findings include interlobular septal thickening with fibrotic bands. CT pertinent negatives are lung nodule, lymphadenopathy and pleural effusion. Yang R et al3 documented that chest CT severity score (CT-SS) could be used to rapidly identify patients with severe forms of COVID-19. CT-SS ranges from 0 to 40 by summing individual scores from 20 lung regions; [scores of 0: 0%, 1: 50%, 2: 50% are respectively assigned for each region according to percentage of parenchymal opacification]. Cutoff >19 signifies severe pneumonia (Figure 2).
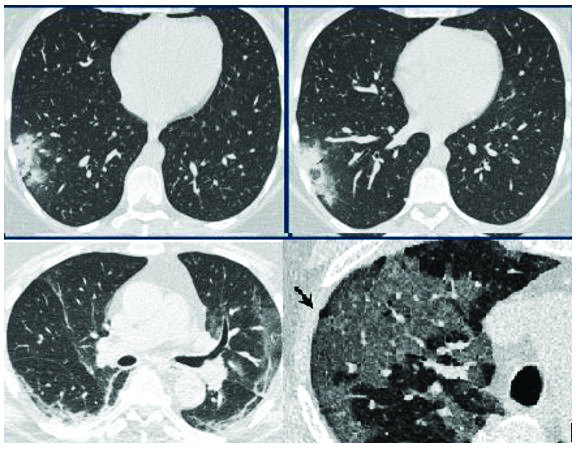
Figure 2: Axial CT sections (lung window) show myriad of parenchy-mal abnormalities in COVID-19.
These imaging tools also help in prognosis, progression and recovery monitoring. But Imaging, like other frontline health departments, is also facing threats of viral exposure to its staff members. As per WHO guidelines, level I and II PPE (gloves, apron, fluid resistant [Type‐IIR] surgical facemasks has been assigned for use by staff members, according to the contact with patients.4,5 Modified portable isolation chamber for imaging, making CT scanner room as a negative pressure room, usage of portable US scanner and X-ray machines are measures to reduce the risk of transmission according to CDC guidelines.6
Globally, where there is high incidence of COVID‐19 like UK, US etc.; one of the departments, CT scanner, is designated as dirty scanner to scan ‘only’ COVID patients. There are specific guidelines issued by Radiological Society of Pakistan for scanner area disinfection including surface wipe of imaging equipment with 75% alcohol solutions +/-H2O2 and surface mop with bleach solution and surf after imaging every COVID‐19 patient. Moreover, during pandemic, numerous online CME’s, webinars and online meetings have been conducted by Radiology Educators all over the world to educate Imaging Physicians and technical staff for self, equipment and Patient protection.
CONFLICT OF INTEREST:
Authors declared no conflict of interest.
AUTHORS' CONTRIBUTION:
MH: Involved in study concepts, designing and editing manus-cript.
AS: Contributed in manuscript preparation and literature search.
REFERENCES
- Shi H, Han X, Jiang N, Cao Y, Alwalid O, Gu J, et al. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infec Dis 2020; 20(4):425-34.
- Salehi S, Abedi A, Balakrishnan S, Gholamrezanezhad A. Coronavirus disease 2019 (COVID-19): A systematic review of imaging findings in 919 patients. AJR Am J Roentgenol 2020; 215(1):87-93.
- Yang R, Li X, Liu H, Zhen Y, Zhang X, Xiong Q, et al. Chest CT severity score: An imaging tool for assessing severe covid-19. Radiology: Cardiothoracic Imaging 2020; 2(2): e200047.
- Cook TM. Personal protective equipment during the COVID‐19 pandemic – a narrative review. Anaesthesia 2020; 75(7):920-7.
- World Health Organization. Rational use of personal protective equipment (PPE) for coronavirus disease (COVID-19): interim guidance, 19 March 2020. World Health Organization; 2020.
- Molton JS, Leek FA, Ng LH, Totman JJ, Paton NI. A novel approach to CT, MR, and examination of patients with infections requiring stringent airborne precautions. Radiology 2016; 278(3):881-7.